doi.org/10.20986/revesppod.2025.1746/2025
CLINICAL CASE
Surgical treatment of first toe necrosis due to septicemia: clinical case
Tratamiento quirúrgico de necrosis del primer dedo por septicemia: caso clínico
Joao Miguel Costa Martiniano1
Rafael Rayo Martín2
Rafael Rayo Rosado2
Sandra Sánchez-Morilla3
Ana M.ª Rayo Pérez2
1Escola Superior de Saúde da Cruz Vermelha Portuguesa. Lisboa, Portugal
2Departamento de Podología. Universidad de Sevilla. España
3Departamento de Enfermería y Podología. Universidad de Málaga. España
Abstract
Septic shock is a critical clinical condition characterized by tissue hypoperfusion and multiorgan failure secondary to a dysregulated host response to infection. One of its most devastating complications is distal ischemic necrosis, which may lead to amputations and severe functional sequelae. In particular, fulminant meningococcal sepsis can cause extensive vascular compromise of the extremities, resulting in irreversible lesions that profoundly affect ambulation and quality of life. We report the case of a 23-year-old woman with a history of meningococcal septic shock who developed partial amputation of the first toe and total amputation of the fifth toe of the right foot, accompanied by painful hypertrophic scarring and biomechanical dysfunction due to rigid plantar flexion of the hallux. A reconstructive procedure was planned to restore forefoot alignment and functionality, consisting of arthrodesis of the first metatarsophalangeal joint, bone reshaping, and soft-tissue reconstruction. Postoperative follow-up included regular clinical assessments, periodic wound care, and the adaptation of a custom silicone digital prosthesis, with both clinical and photographic documentation until discharge. Reconstruction of the first ray through arthrodesis and surgical remodeling, complemented by functional rehabilitation and prosthetic support achieved recovery of an ergonomic gait pattern, complete pain relief, and significant improvement in foot function. This case underscores the effectiveness of a comprehensive reconstructive approach in managing ischemic necrosis sequelae following meningococcal sepsis.
Keywords: Septic shock, sepsis, treatment, necrosis, ischemia, foot, toes, arthrodesis
Abstract
Septic shock is a critical clinical condition characterized by tissue hypoperfusion and multiorgan failure secondary to a dysregulated host response to infection. One of its most devastating complications is distal ischemic necrosis, which may lead to amputations and severe functional sequelae. In particular, fulminant meningococcal sepsis can cause extensive vascular compromise of the extremities, resulting in irreversible lesions that profoundly affect ambulation and quality of life. We report the case of a 23-year-old woman with a history of meningococcal septic shock who developed partial amputation of the first toe and total amputation of the fifth toe of the right foot, accompanied by painful hypertrophic scarring and biomechanical dysfunction due to rigid plantar flexion of the hallux. A reconstructive procedure was planned to restore forefoot alignment and functionality, consisting of arthrodesis of the first metatarsophalangeal joint, bone reshaping, and soft-tissue reconstruction. Postoperative follow-up included regular clinical assessments, periodic wound care, and the adaptation of a custom silicone digital prosthesis, with both clinical and photographic documentation until discharge. Reconstruction of the first ray through arthrodesis and surgical remodeling, complemented by functional rehabilitation and prosthetic support achieved recovery of an ergonomic gait pattern, complete pain relief, and significant improvement in foot function. This case underscores the effectiveness of a comprehensive reconstructive approach in managing ischemic necrosis sequelae following meningococcal sepsis.
Keywords: Septic shock, sepsis, treatment, necrosis, ischemia, foot, toes, arthrodesis
Corresponding author
Rafael Rayo Martín
rafaelrayo@us.es
Received: 16-07-2025
Accepted: 07-10-2025
Introduction
Septic shock is a severe clinical entity characterized by systemic tissue hypoperfusion, organ dysfunction, and cellular death secondary to a dysregulated host response to infection(1,2). Among its clinical forms, fulminant meningococcal sepsis represents one of the most devastating presentations, as it can rapidly progress to multiorgan failure and purpura fulminans with severe peripheral vascular compromise(3,4). This microvascular involvement can lead to ischemia and distal necrosis, resulting in digital or even complete limb amputations, with major anatomic and functional consequences in young, previously healthy patients. Thromboembolic complications observed in meningococcal shock are related to the direct toxic effects of Neisseria meningitidis on tissues, disseminated intravascular coagulation, and the release of vasoactive cytokines that alter microcirculation5. Although rare, tissue necrosis associated with this condition mainly affects the lower limbs and usually manifests as multifocal ischemic lesions that progressively coalesce(5,6).
After the acute phase of septic shock, one of the main challenges lies in the management of orthopedic sequelae resulting from previous non-standard or nonfunctional amputations(4). These situations often lead to a dysfunctional forefoot, characterized by biomechanical alterations, residual pain, and gait difficulties, which severely impact quality of life. Current literature offers limited insight into reconstructive procedures aimed at restoring forefoot alignment and optimizing function following partial amputations secondary to septic ischemic necrosis, representing a significant knowledge gap(5,6,7). Describing effective surgical strategies to address these sequelae is crucial to improve functional recovery and prevent long-term complications.
The present article presents the case report of a young female patient with a past medical history of meningococcal septic shock who developed digital amputations and a dysfunctional forefoot, treated by atypical metatarsophalangeal arthrodesis and structural reconstruction of the first ray. The objective is to describe the surgical and functional approach used, as well as the clinical course and outcomes, providing evidence on a viable reconstructive option for complex postischemic sequelae. This article was prepared following the CARE (CAse REport) guidelines for case report presentation and development in scientific journals(8).
Case report
in September 2021, a 23-year-old woman presented with a history of digital amputations resulting from an episode of meningococcal septic shock. The patient reported disabling pain in the right great toe, particularly during ambulation, described as a “stabbing” sensation in the distal hallux region, significantly impairing walking function and ergonomics.
Her past medical history included congenital facial and cardiac anomalies, with closure of a patent foramen ovale at age seven. In 2013, she was diagnosed with a 2-cm intestinal neuroendocrine tumor, treated by resection of one-third of the large intestine. She had no known allergies and was not on any drugs at the time of consultation. In 2015, she experienced meningitis progressing to septic shock (Figure 1), leading to severe distal ischemia in both lower limbs, more pronounced in the right foot. During this episode, three surgical debridements of necrotic tissue were performed (April, May, and June 2015). As sequelae, the patient presented partial amputation of the right hallux at the proximal phalanx and total amputation of the right fifth toe, with a painful hypertrophic scar in the lateral area. The left foot showed partial distal amputation of the second and third toes, with good healing and no pain.

Clinical examination (Figure 2) of the right foot revealed a rigid first metatarsophalangeal joint, with the hallux in fixed plantar flexion and absence of the distal phalanx, producing a painful stump and altered propulsion during gait. The deformity was interpreted as a result of postamputation shortening and cicatricial fibrosis of the residual flexor, with no distal traction. Direct pressure elicited pain over the residual tip of the first toe, which was deformed but retained limited joint mobility. The right fifth toe had a painful hypertrophic scar with a residual corn secondary to total amputation. The left foot showed normotrophic scars at the partial amputation sites of the second and third toes, with no pain or plantar overload, thus requiring no surgery.

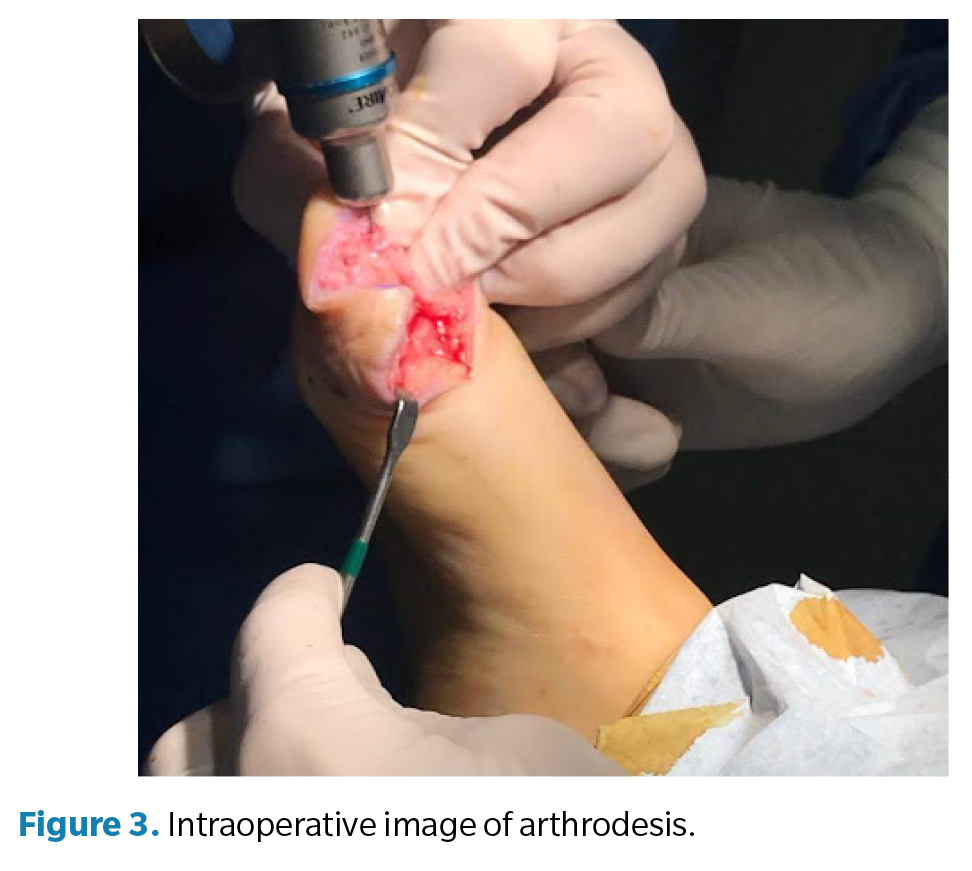
Surgery (Figure 3) was performed in March 2022 under regional anesthesia using a posterior popliteal block and conscdious sedation supervised by an anesthesiologist. Antibiotic prophylaxis with 2 g of IV cefazolin was administered 30 minutes before incision, and a pneumatic ankle tourniquet was applied (250 mm Hg), with controlled pressure and ischemia time limited to 45 minutes. A longitudinal dorsal approach to the first metatarsophalangeal joint was performed, preserving neurovascular structures. Irregular bony remnants of the proximal phalanx were identified and completely resected, followed by contouring of bone margins to achieve smooth, viable surfaces. Articular surfaces of the first metatarsophalangeal joint were then prepared by burring and curettage until an adequate bleeding base for arthrodesis was obtained. Fusion position was determined intraoperatively under load testing, fixing the hallux at approximately 10° dorsiflexion relative to weightbearing surface to optimize propulsion and prevent plantar overload on the residual stump. Final fixation was achieved using one cannulated compression screw, ensuring intraoperative stability and correct alignment under fluoroscopy (Figure 4). The procedure concluded uneventfully, with meticulous hemostasis and layered closure.

The postoperative period included periodic dry dressings and progressive functional follow-up. At 3 months, complete pain resolution and significant improvement in gait quality were observed. At 6 months, the patient showed satisfactory functional recovery, allowing temporary medical discharge. Customized silicone digital prostheses were later fabricated for both feet to improve podiatric symmetry, load distribution, and psychosocial acceptance. At 12-month follow-up, the patient remained asymptomatic, with complete radiographic consolidation of the arthrodesis, correct alignment of the first ray, and stable gait without limitations, confirming the functional success of the procedure.
Discussion
Vascular and tissue sequelae following septic shock represent a complex therapeutic challenge, particularly when they result in cutaneous necrosis and distal amputations. In this case, a young woman experienced severe right foot sequelae due to meningococcal septic shock, leading to distal ischemia, multiple debridements, and digital amputations, including critical hallux involvement. This clinical scenario is not uncommon and has been reported in several contexts of severe sepsis, where vasopressor use, sepsis-induced coagulopathy, and the virulence of the infectious agent contribute to irreversible peripheral vascular compromise(9,10).
Cutaneous and tissue necrosis associated with prolonged vasopressor use has been described as a frequent complication in critically ill patients10. In our case, despite initial attempts at tissue salvage, the patient developed irreversible lesions that resulted in partial amputations and loss of first-ray function. This pattern aligns with that described by Chen et al. (11), who proposed the concept of “physiologic cryoamputation” as a conservative strategy to allow natural demarcation of necrotic tissue before definitive surgery.
The hallux plays a fundamental role in propulsion and stability during gait, and its deformity or loss significantly alters foot biomechanics(12,13,14). In this patient, persistent residual pain due to plantar overload in the amputated segment required first metatarsophalangeal arthrodesis. Unlike standard arthrodesis without amputation history, this technique required careful remodeling of irregular phalangeal remnants and intraoperative selection of the fusion position (approximately 10° dorsiflexion). This technical detail was essential to prevent recurrent overload on the residual stump and restore functional support. Although technically not more difficult than a conventional arthrodesis, adjusting fusion position to an amputated segment represented the main procedural modification.
Sequential reconstructive strategies are supported by the literature. Henn et al. (15) reported cases of limb reconstruction after vasopressor-induced ischemia, prioritizing restoration of functional axis and aesthetics. Similarly, the additional use of silicone digital prostheses, as in this case, has demonstrated benefits in podiatric symmetry, load distribution, and psychosocial acceptance. This aesthetic-functional component is particularly relevant in young patients, for whom the psychological impact of amputation can be substantial(16,17).
Similar cases have been described in infections caused by Vibrio vulnificus, Aeromonas spp., and even SARS-CoV-2(14,18), all sharing a common pathophysiologic pattern: severe microangiopathy, endothelial activation, and distal vascular compromise leading to irreversible amputations. These reports reinforce the notion that, regardless of the etiologic agent, management should focus on functional reconstruction and comprehensive rehabilitation once ischemia is established.
Finally, long-term follow-up is essential to evaluate the success of such interventions. In this case, 12-month follow-up confirmed complete arthrodesis consolidation, absence of pain, and restoration of physiological gait, supporting the effectiveness of the chosen approach.
In conclusion, this case highlights the importance of personalized reconstructive techniques in patients with sequelae of septic shock. Functional hallux arthrodesis, combined with bone remodeling, soft-tissue reconstruction, and silicone digital prostheses, allowed both functional and aesthetic restoration of the foot. This experience underscores the need of a prolonged follow-up, individualized surgical planning to optimize clinical and psychosocial outcomes in this patient population.
Conflict of interest
None declared
Funding
None declared
Contributions of the authors
Study conception and design: R.R.S. Data collection: R.R.M. Analysis and interpretation of results: S.S.M. Drafting and manuscript preparation: A.M.R.P. Final review: J.M.C.M.
References
- Olgemöller U, Becker C. [Septic shock]. Dtsch Med Wochenschr. 2025;150(7):333-41. German. DOI: 10.1055/a-2288-2366.
- Singer M, Deutschman CS, Seymour CW, Shankar-Hari M, Annane D, Bauer M, et al. The third international consensus definitions for sepsis and septic shock (Sepsis-3). JAMA. 2016;315(8):801-10. DOI: 10.1001/jama.2016.0287.
- Durán Giménez-Rico HJ, Aller Reyero MA, Lorente Ruigómez L, Durán Giménez-Rico L, Arias Pérez J, Durán Sacristán H. Sepsis y shock séptico: un torbellino de mediadores inflamatorios de difícil manejo terapéutico. An Med Interna. 2002;19(1):35-43.
- Landham TL, Datta D, Nirula HC. Amputation for gangrene of the limbs following severe meningococcal infection. J R Coll Surg Edinb. 1991;36:11-2.
- Pacheco Pacori YD, García Duque O. Necrosis isquémica de todos los dedos y ortejos después del uso de norepinefrina en paciente ginecológico. An Fac Med. 2018;79(2):149-52.
- González Aguilera JC, Mengana Medina MD, Vázquez Belizón YE, Dorta Rodríguez E, Algas Hechavarría LA. Manifestaciones cutáneas por choque séptico en una adulta. MEDISAN. 2015;19(5):639-45.
- Casteleiro Roca P, Midón Miguez J, García Barreiro J, Martelo Villar F. Tratamiento quirúrgico de las complicaciones del shock meningocóccico grave. Cir Plást Iberolatinoam. 2010;36(2):155-62.
- Red Caspe. Materiales y herramientas para la investigación. Disponible en: https://redcaspe.org/materiales/. Acceso mayo de 2025.
- Ruffin N, Vasa CV, Breakstone S, Axman W. Symmetrical peripheral gangrene of bilateral feet and unilateral hand after administration of vasopressors during septic shock. BMJ Case Rep. 2018;2018:bcr2017223602. DOI: 10.1136/bcr-2017-223602.
- García Harana C, Fernández Canedo I, de Troya Martín M. Skin necrosis after septic shock. Med Clin (Barc). 2019;152(3):e17. DOI: 10.1016/j.medcli.2018.04.005.
- Chen SL, Kuo IJ, Kabutey NK, Fujitani RM. Physiologic cryoamputation in managing critically ill patients with septic, advanced acute limb ischemia. Ann Vasc Surg. 2017;42:50-5. DOI: 10.1016/j.avsg.2016.11.006.
- Morandi EM, Pauzenberger R, Tasch C, Rieger UM, Pierer G, Djedovic G. A small ‘lick’ will sink a great ship: Fulminant septicaemia after dog saliva wound treatment in an asplenic patient. Int Wound J. 2017;14(6):1025-8. Doi: 10.1111/iwj.12752.
- Pan Z, Guo X, Huang P, Duan L, Hong W, Xie YW, et al. Early diagnosis and application of hemopurification combined with antibiotic therapy and surgical debridement for successful treatment of a child with Vibrio vulnificus necrotizing fasciitis and septic shock: A case report. BMC Infect Dis. 2025;25(1):286. DOI: 10.1186/s12879-025-10691-2.
- Henn MC, Hathaway BA, Lipira AB. Reconstructive surgical management of vasopressor-ischemia related distal extremity loss. J Orthop Case Rep. 2025;15(4):45-51. DOI: 10.13107/jocr.2025.v15.i04.5440.
- Leechavengvongs S, Jidpugdeebodin S, Milindankura S. Necrotising fasciitis causing compartment syndrome of the forearm and septic shock due to Vibrio vulnificus: A case report. Hand Surg. 2006;11(1-2):77-82. DOI: 10.1142/S0218810406003164.
- Bhatia N, Castro-Borobio M, Greene JN, Nanjappa S. Necrotizing fasciitis secondary to Aeromonas infection presenting with septic shock. Case Rep Med. 2017;2017:4607582. DOI: 10.1155/2017/4607582.
- Shin JY, Roh SG, Lee NH, Yang KM. Ischemic necrosis of upper lip and all fingers and toes after norepinephrine use. J Craniofac Surg. 2016 Mar;27(2):453-4. DOI: 10.1097/SCS.0000000000002463.
- Pinzon D, Baumgarten D, Galetke W. 39-jährige Frau mit schwerer COVID-19-Pneumonie: Erfolgreiches Weaning nach septischem Schock und Vorfußamputation wegen mikrovaskulärer Komplikationen [39-year-old woman with severe COVID-19 pneumonia: successful weaning after septic shock and forefoot amputation after microvascular complications]. Pneumologie. 2021 ;75(7):526-30.