doi.org/10.20986/revesppod.2025.1762/2025
ORIGINAL
Comparative observational analysis between the beighton test and the Foot and Ankle Flexibility Index (FAFI) in a sample of the extremadian pediatric population
Análisis observacional comparativo entre el test de beighton y foot and ankle flexibility index (fafi) en una muestra de población pediátrica extremeña
Noelia García Lorenzo1
Paula Cobos Moreno1
Beatriz Gómez Martín1
1Centro Universitario de Plasencia. Cáceres. España
Abstract
Introduction: Flexible flatfoot in children is a common condition during childhood, considered in most cases a physiological variant of development. However, in some instances, it may persist and progress into pathological forms that affect the child’s quality of life. This research arises from the need to establish objective clinical criteria to differentiate between a benign developmental variant and a condition with pathological potential. The main objective of this study is to examine the comparison between the Beighton Test and the Foot and Ankle Flexibility Index (FAFI) in the population of Extremadura.
Patients and methods: A correlation was found between the Beighton Test and the FAFI. The comparison between both assessment tools showed that they yield consistent results in detecting joint hypermobility.
Results: A correlation was found between the Beighton Test and the FAFI (p < 0.001). The comparison between both assessment tools showed that they yield consistent results in detecting joint hypermobility.
Conclusions: The study concludes that there is a positive correlation between the Beighton Test and the FAFI. The complementary use of both instruments may represent a robust methodological approach for a more thorough and accurate assessment of joint hyperlaxity, particularly in the distal segment of the lower limbs.
Keywords: Flexible flatfoot, joint hypermobility, Body Mass Index, Foot Posture Index, Foot and Ankle Flexibility Index, pediatric population, podiatry
Resumen
Introducción: El pie plano flexible infantil es una condición común durante la infancia, considerada en la mayoría de los casos como una variante fisiológica del desarrollo. No obstante, en algunos casos puede persistir y evolucionar hacia formas patológicas que afectan la calidad de vida del menor. Esta investigación surge ante la necesidad de establecer criterios clínicos objetivos que permitan diferenciar entre una variante benigna del desarrollo y una alteración con potencial patológico. El objetivo principal del trabajo es examinar la comparación entre el test de Beighton y el Foot and Ankle Flexibility Index (FAFI) en la población extremeña.
Pacientes y métodos: Se llevó a cabo un estudio observacional, descriptivo y transversal en 78 escolares. A todos los sujetos del estudio se les realizaron diversas pruebas clínicas podológicas: escala de Beighton y FAFI.
Resultados: Sí existe una correlación entre el test de Beighton y el FAFI (p < 0.001). La comparación entre ambas herramientas de evaluación ha evidenciado que ambas presentan resultados concordantes en la detección de hipermovilidad articular.
Conclusiones: El estudio concluye que sí existe una correlación positiva entre el test de Beighton y el FAFI. La aplicación complementaria de ambos instrumentos podría constituir un enfoque metodológico importante para una evaluación más exhaustiva y precisa de la hiperlaxitud articular, particularmente en el segmento distal de las extremidades inferiores.
Palabras claves: Pie plano flexible, hipermovilidad articular, Índice de Masa Corporal, Índice de Postura del Pie, Índice Flexibilidad Pie y Tobillo, población infantil, podología
Corresponding author
Paula Cobos Moreno
pacobosm@unex.es
Received: 19-09-2025
Accepted: 09-10-2025
Introduction
Flexible flatfoot is one of the most common morphological alterations in childhood. It is characterized by the loss or reduction of the medial longitudinal arch when the child adopts a standing position, with recovery of the arch once the weight load is removed. Although in most cases it forms part of normal physiological development, related to the immaturity of osteoarticular and muscular structures(1,2)., it does not always resolve spontaneously. In some individuals, it may persist or progress to more severe forms, causing pain, functional limitations, and difficulties performing sports or daily activities, thus justifying the need for adequate clinical assessment(3)..
The management of flexible flatfoot in childhood poses a challenge for health care professionals, as it is essential to differentiate between a normal developmental variant and an alteration that may lead to long-term biomechanical problems. Recent literature highlights that, although in most children this condition is asymptomatic, in certain cases it may manifest as discomfort after prolonged physical activity or even progress to painful conditions during adolescence and adulthood, negatively affecting quality of life(4,5.. This context has sparked growing interest within the podiatric community, aiming to establish more precise diagnostic criteria to identify at-risk populations and offer early interventions when necessary(3)..
Among the factors associated with flexible flatfoot, joint hypermobility plays a relevant role(3,6).. Reduced structural stiffness favors deformation of the plantar arch under load, increasing the likelihood of flatfoot persisting or worsening. Therefore, assessing joint hypermobility in the pediatric population is of great importance—not only for diagnosis but also for preventing potential biomechanical complications in later stages.
For this assessment, the Beighton test has become the most widely used tool in both clinical and research settings(7).. However, this test presents limitations, as it provides only a general approximation of joint laxity without specifically addressing the foot–ankle complex, which is crucial in flexible flatfoot. In this regard, the Foot and Ankle Flexibility Index (FAFI) has emerged as a recent alternative, designed specifically to measure foot and ankle flexibility. Its application could provide more detailed and clinically useful information in pediatric contexts(8,9º)..
Consequently, the present study aims to compare the usefulness of the Beighton test and the FAFI in the pediatric population of Extremadura to determine which provides a more comprehensive assessment of joint hypermobility in relation to flexible flatfoot. The ultimate goal is to provide evidence that contributes to optimizing clinical practice and advancing scientific knowledge in pediatric podiatry, thereby improving identification of patients who may benefit from specific monitoring or treatment.
Patients and methods
Study type and sample size
According to Argimón Pallàs and Jiménez Villa10, the present study is cross-sectional, observational, and descriptive. The study population consisted of 78 children aged 6–7 years, with a mean age of 6.13 ± 0.336 years, including 41 boys (52.6 %) and 37 girls (47.4 %), showing a relatively balanced distribution between sexes. Participants were recruited from various public and private schools located in the municipality of Plasencia (Cáceres, Spain). Data collection was conducted between January and March 2025.
The inclusion criteria are: boys and girls aged 6–7 years; subjects presenting with flexible flatfoot.
The exclusion criteria are: subjects with a body mass index ≥ 30 kg/m², compatible with excess weight load on the foot; children with genetic, neurological, inflammatory, or muscular disorders, or with morphological and/or functional alterations of the foot; individuals currently undergoing podiatric treatment, such as plantar orthoses or therapeutic footwear, among others.
Procedure
All subjects underwent several clinical tests: Beighton scale and FAFI, following previously established and standardized clinical criteria, to minimize inter- and intra-examiner bias.
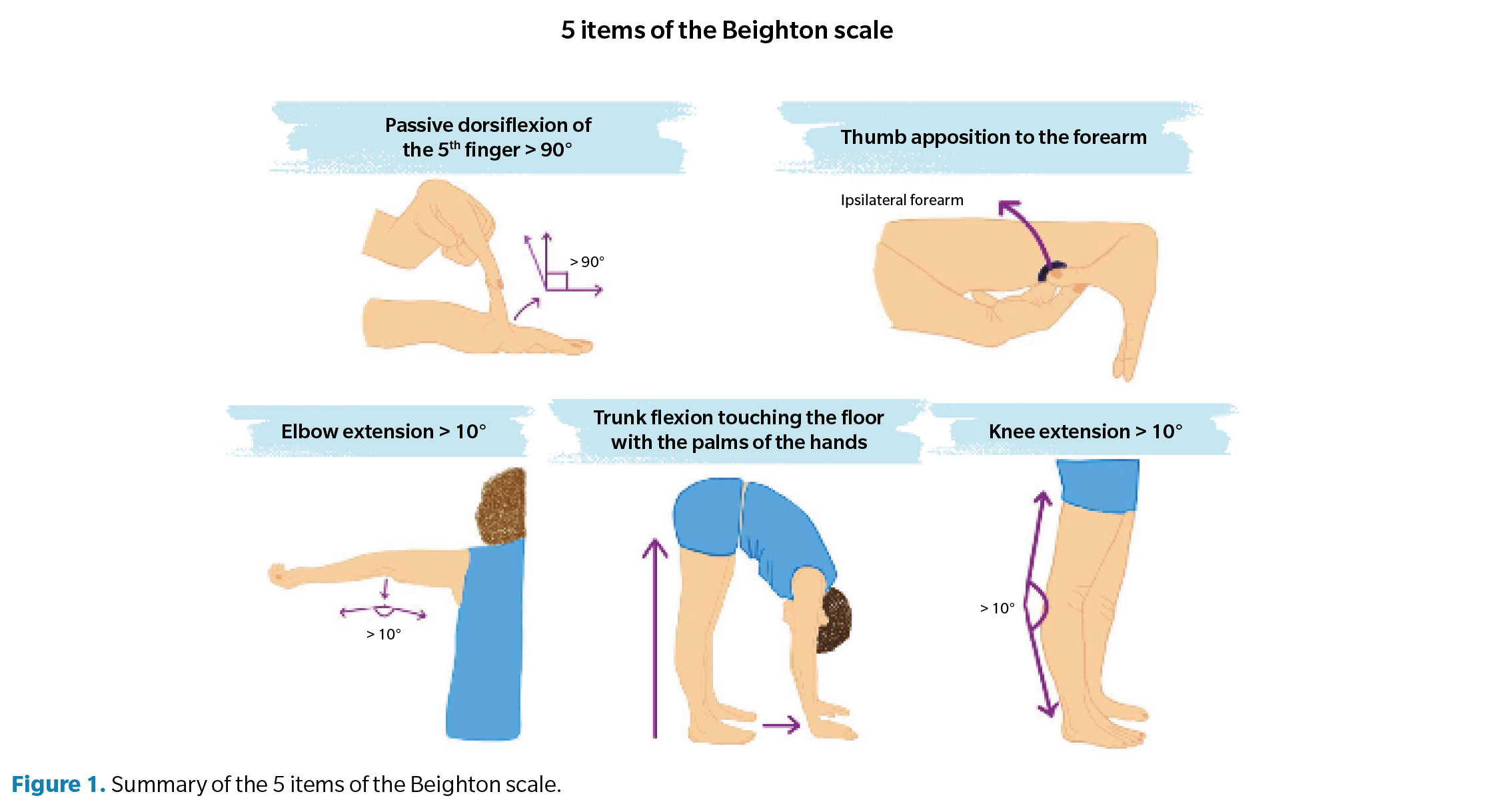
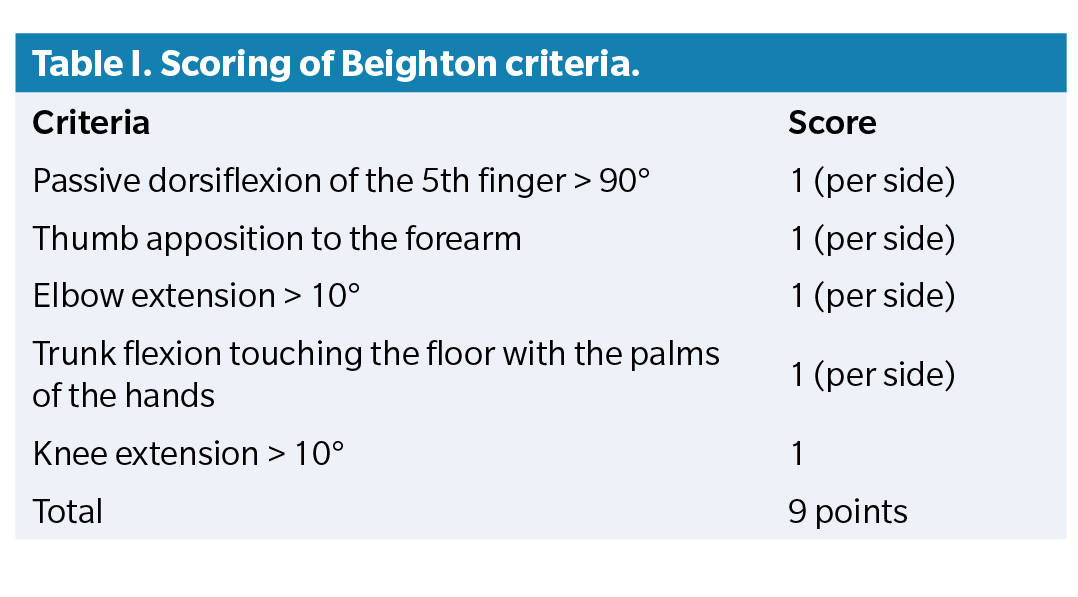
The Beighton scale consists of 5 items assessing joint hypermobility, as shown in Figure 1 and Table 1. Each item is scored bilaterally (0 = negative, 1 = positive), yielding a total score ranging from 0 to 9. Recent studies recommend using age-, sex-, and group-adjusted cut-off values. In children, generalized joint hypermobility is considered present when the score is ≥ 6¹¹.
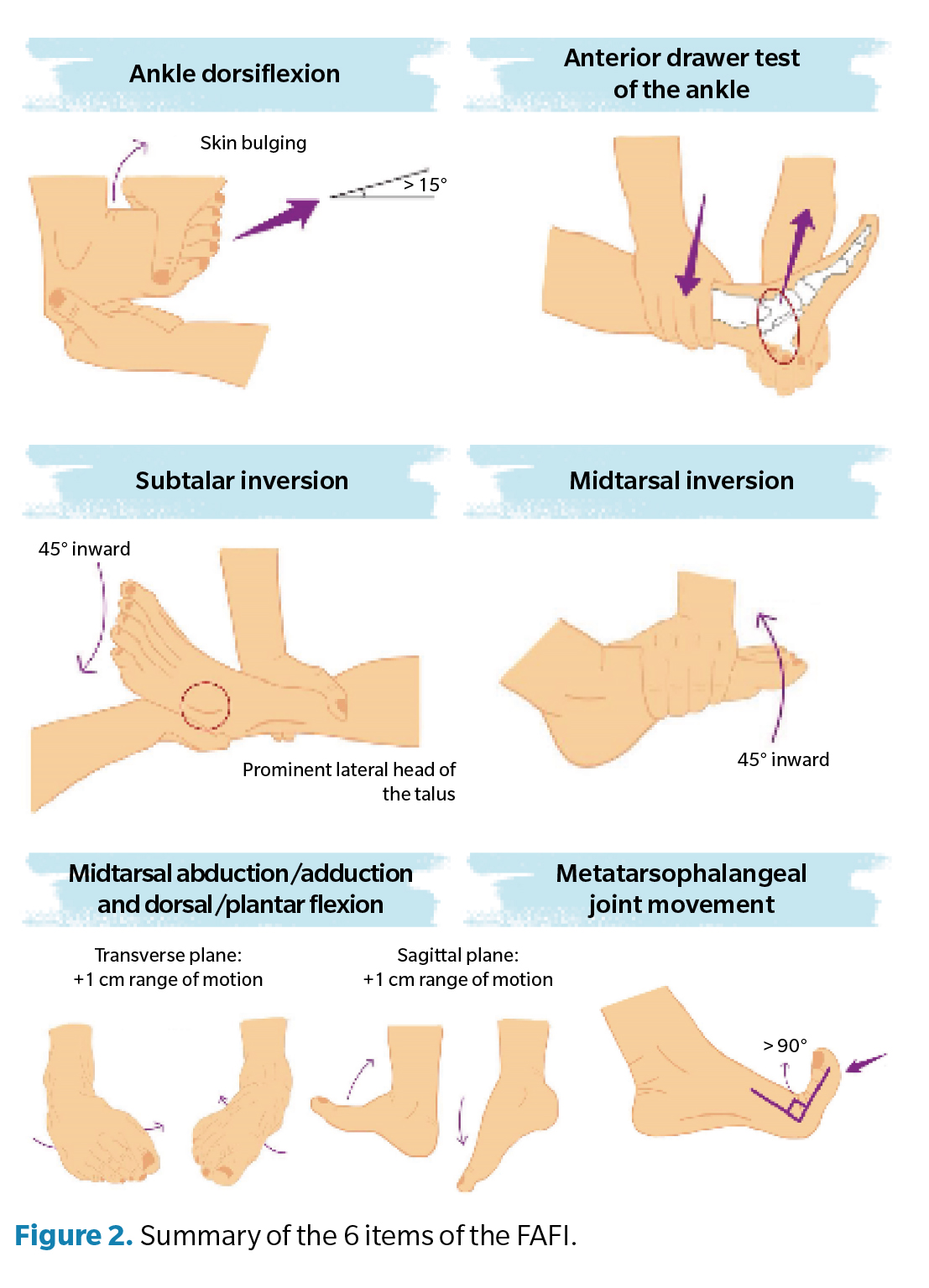
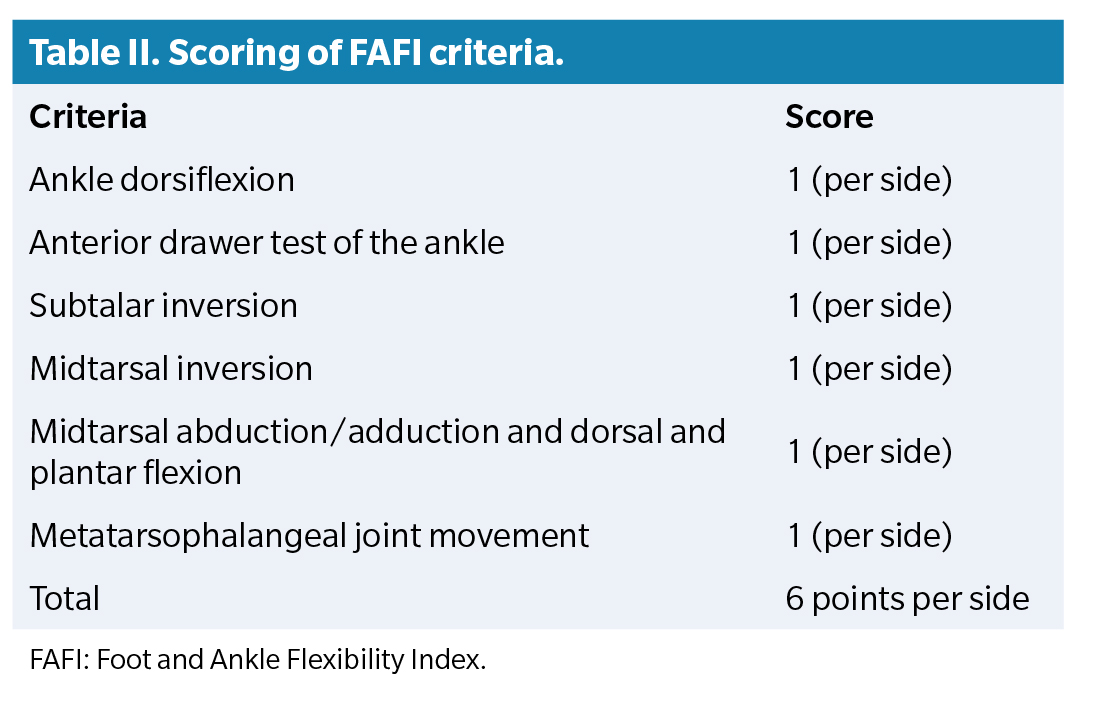
The FAFI assesses joint hypermobility through 6 items (Figure 2, Table 2). Each foot is evaluated independently, assigning separate scores for the left and right sides (0 = negative, 1 = positive). The total score for each foot ranges from 0 to 6. According to recent studies, a score ≥ 4/6 suggests hypermobility of the foot and ankle(12)..
Data for this study were obtained through podiatric examination of participants, conducted in classrooms provided by the participating schools. Data were collected using a specific form designed for this purpose and subsequently entered into Microsoft Excel for digital organization and later statistical analysis.
Statistical analysis
Data analysis was performed using SPSS software (version 21.0 for iOS). Hippothesis testing was performed using inferential statistical tools that were non-parametric tests, given that the variables were qualitative or quantitative without a normal distribution pattern. First, data normality was assessed using the Kolmogorov–Smirnov test. To analyze relationships between quantitative variables, the Kruskal–Wallis test was used to compare distributions between independent groups. The Wilcoxon signed-rank test was applied to compare two related samples, and the Mann–Whitney U test for independent variables. Finally, Spearman’s rank correlation coefficient was used to measure relationships between numerical variables. Five percent value (p < 0.05) was used as the limit for statistical significance in the contrast hypothesis testing.
Results
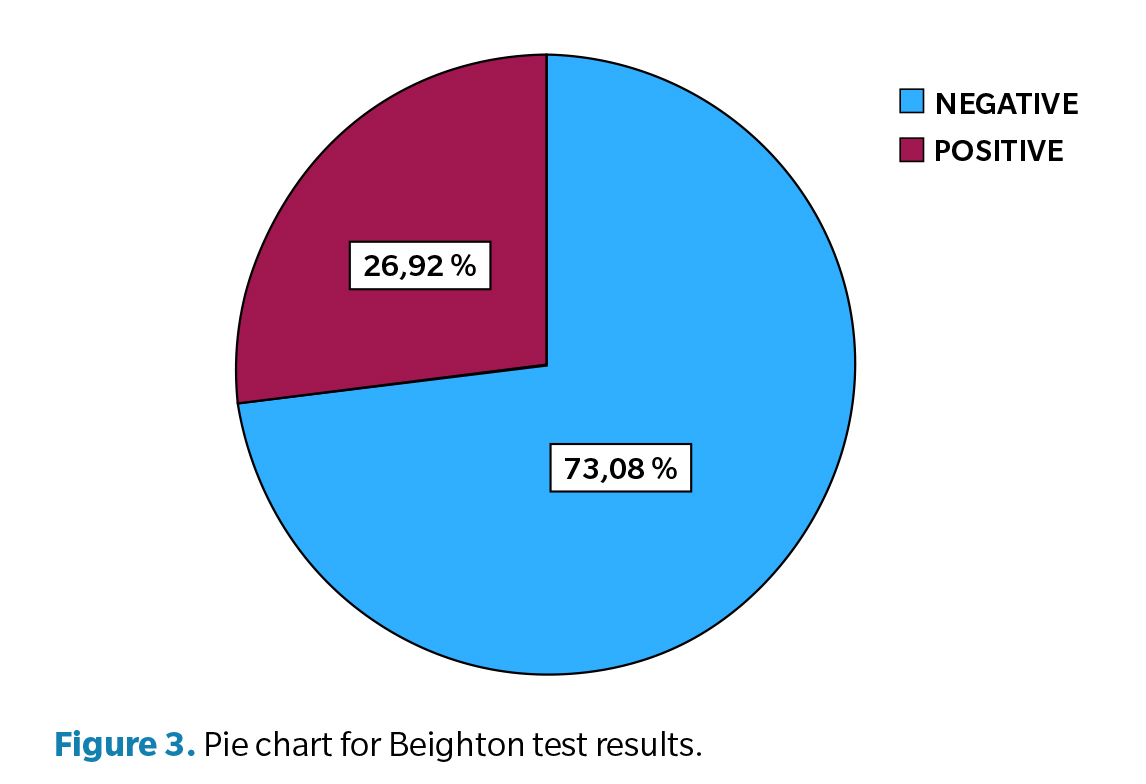
The Beighton scale data did not follow a normal distribution (p < 0.001, Kolmogorov–Smirnov); therefore, non-parametric statistical tests were used. In the sample of 78 children, Beighton scores were distributed as follows (Figure 3): 57 children (73.1 %) obtained negative results, indicating absence of significant hypermobility. 21 children (26.9 %) showed positive results, suggesting the presence of joint hypermobility.
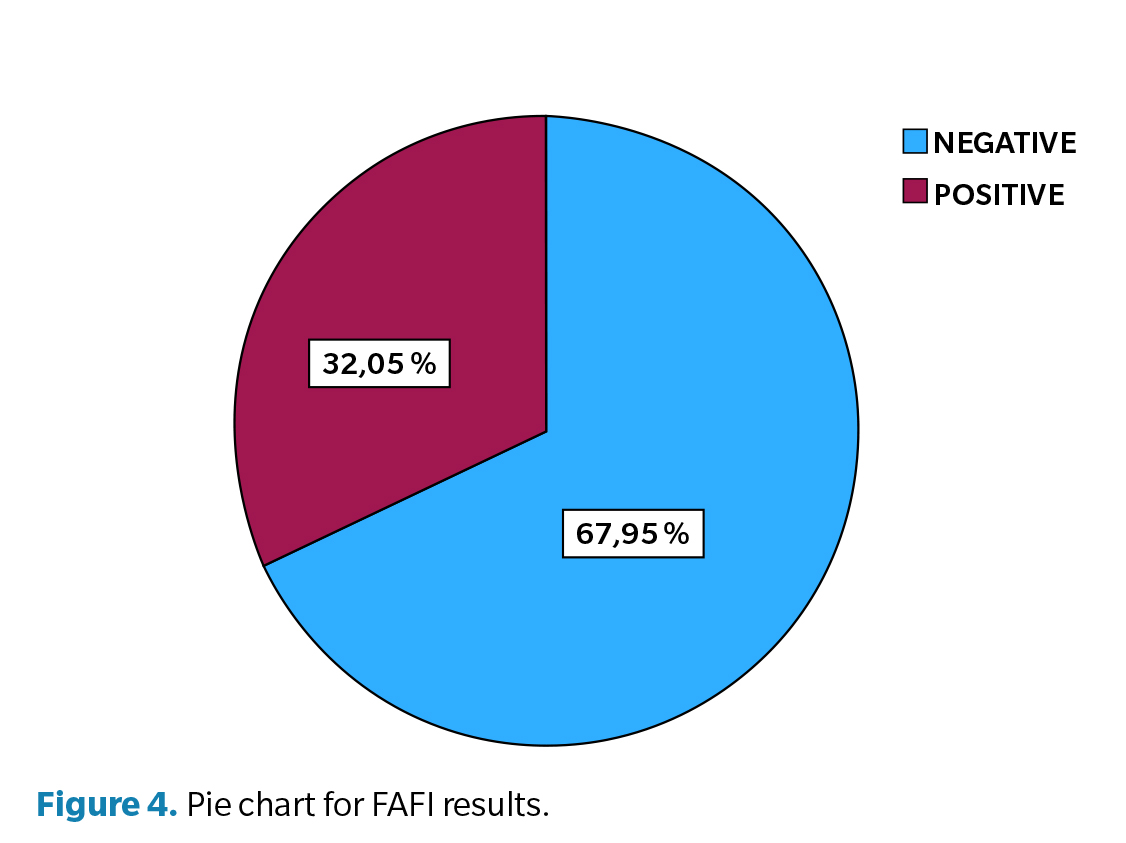
Regarding FAFI results (Figure 4), 32.05 % of children showed positive results, while 67.95 % showed negative results. These findings indicate that most children presented FAFI values within a normal functional range.
To determine whether an association existed between foot–ankle flexibility (FAFI) and joint hypermobility (Beighton), a Mann–Whitney U test was applied. Results indicated a statistically significant difference (p < 0.001), suggesting that foot–ankle flexibility varies according to the presence or absence of hypermobility.
Additionally, non-parametric correlation analysis (Spearman’s p) confirmed this relationship with a correlation coefficient of 0.370 (p < 0.001), indicating a moderate-to-low association between both variables. This means that children with greater hypermobility tend to present differences in foot and ankle flexibility compared to those without hypermobility.
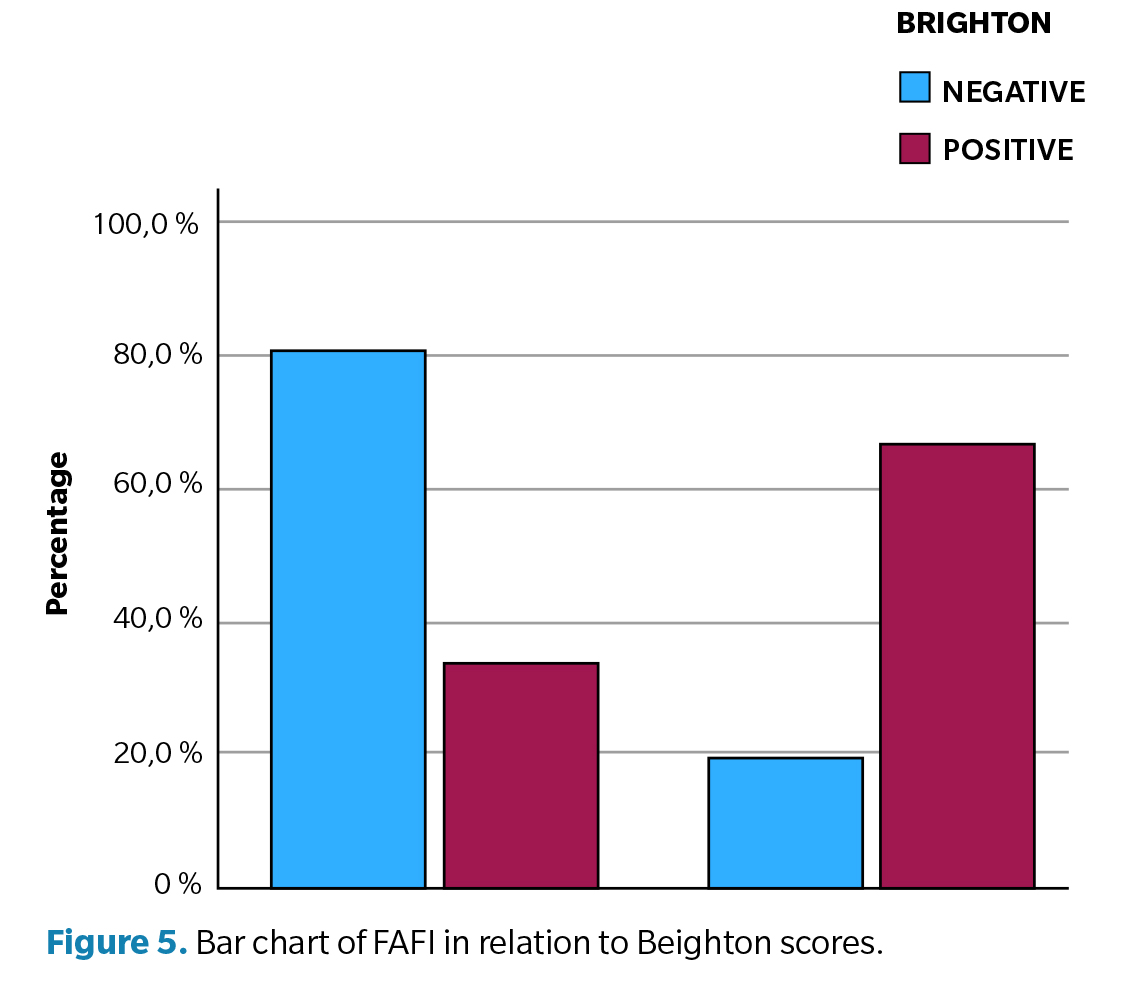
Figure 5 further supports this finding among children with negative FAFI, 80.7 % showed no hypermobility (Beighton negative), while 19.3 % did (Beighton positive). Among those with positive FAFI, 33.3% showed no hypermobility, compared to 66.7% who did.
The association between foot and ankle flexibility (FAFI) and joint hypermobility (Beighton test) can also be supported by the relationship map shown in Figure 6, which shows how certain levels of one variable tend to be linked with specific values of the other.
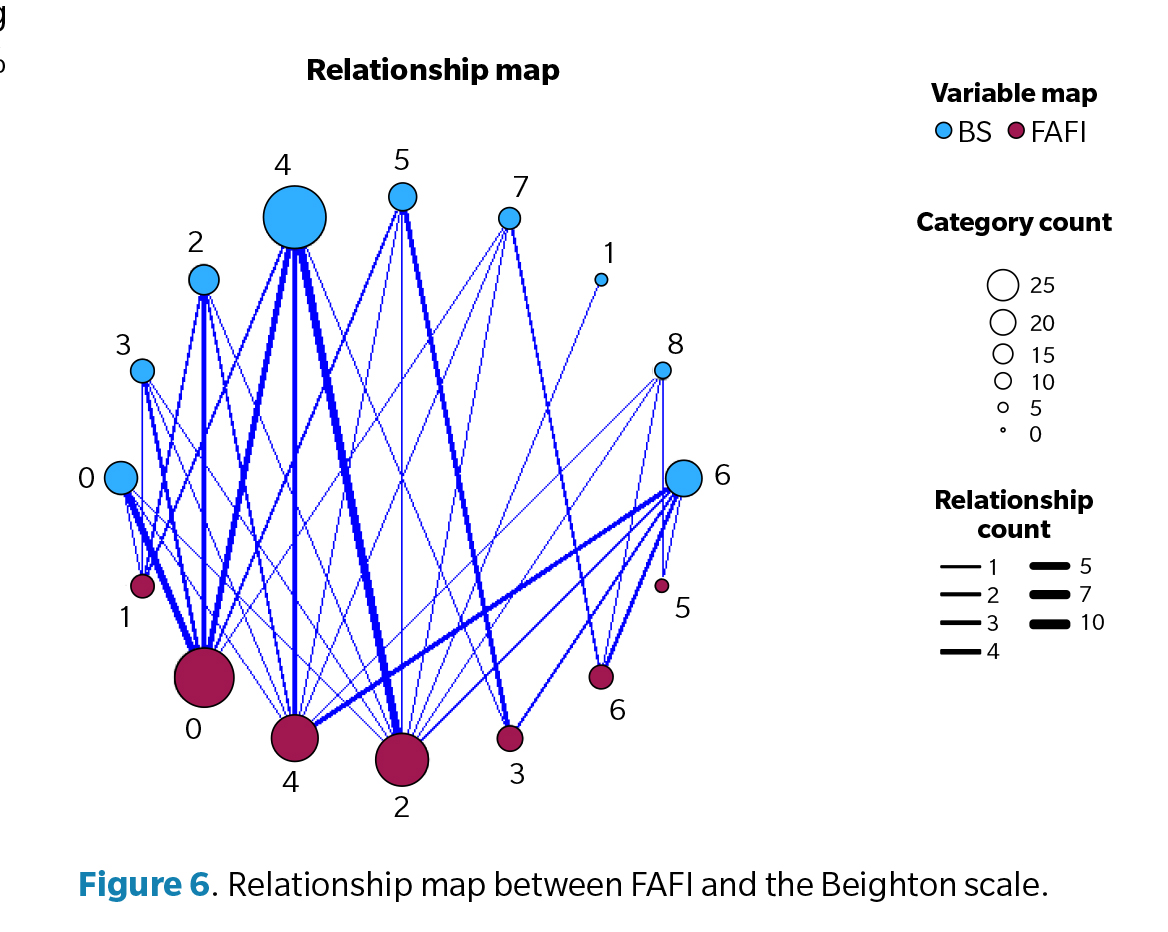
Multiple connections can be observed between different FAFI values and Beighton scale scores in the map. Some Beighton nodes (blue circles), such as scores 4 and 6, have thicker connections with several FAFI values, indicating that these hypermobility levels are more common at certain degrees of foot–ankle flexibility. Smaller nodes represent fewer individuals in those categories and therefore fewer connections.
Discussion
The results obtained in the present study show that 26.9 % of the children evaluated presented joint hypermobility according to the criteria established by the Beighton test. In contrast, 73.1 % obtained a negative result, meaning they did not present hypermobility according to the same test. These results fall within the range reported in the scientific literature by Engelbert and Rombaut(11)., which varies between 7 % and 36 % in the pediatric population (children and adolescents). Therefore, the findings obtained in this study are consistent with those previously described in other works, reinforcing the validity of the results and situating the analyzed sample within the expected parameters.
Similarly, these results emphasize the importance of continuing to use standardized tools such as the Beighton test for the detection of hypermobility at early ages. The results obtained in the analysis of joint hypermobility in the foot and ankle through the application of the FAFI show that 67.95 % of the children evaluated presented a negative result, while 32.05 % obtained a positive result for joint hypermobility in these joints. Since the FAFI is a recently developed evaluation tool in the scientific context and considering the limited literature available using this instrument, it has not been possible to establish direct comparisons with previous studies. This lack of background reinforces the need to continue research in this area to generate a solid database that allows the validation and consolidation of its clinical and academic use.
Of note, relevance of incorporating the FAFI as a specific and standardized instrument for identifying joint hypermobility in the foot–ankle complex. It is a tool that has demonstrated reliability and validity, making it a valuable resource both for clinical assessment and for designing future research focused on the functional and biomechanical characteristics of the foot and ankle in childhood.
Regarding the correlation between both evaluation tools (Beighton scale–FAFI), a relationship was observed between them. The comparison between the Beighton scale and the FAFI showed that both instruments yielded concordant results in the detection of joint hypermobility.
However, it was identified that the Beighton test provides a global assessment of body flexibility, while the FAFI may offer a more specific evaluation focused on the functionality and flexibility of the foot–ankle complex. This difference in focus suggests that the combined use of both instruments could be a useful strategy to achieve a more complete and accurate evaluation of joint hypermobility, especially in the distal region of the lower limbs.
As mentioned previously, the FAFI is a newly introduced evaluation tool in the scientific field. Given the limited existing literature supporting its use, it has not been possible to make direct comparisons with a significant number of prior studies. Notably, the works of Martínez-Sebastián et al. (8,9).point out that “in half of the cases in which the FAFI was positive, the Beighton test did not identify joint hypermobility,” which reinforces the hypothesis that the combined use of both tools improves diagnostic capacity, considering that the Beighton scale does not include any specific items for assessing the foot and ankle.
Among the most relevant limitations of this study are the relatively small sample size, which restricts the generalization of the results to other pediatric populations. In addition, the limited prior scientific literature on the use of the FAFI in this context makes it difficult to compare the findings obtained, which limits its external validation. Similarly, the observational design of the study does not allow for establishing causal relationships between the analyzed variables. These limitations highlight the need to continue research in this area, through studies with larger samples and comparative methodologies to consolidate the use of the FAFI as a valid and reliable clinical tool.
Nevertheless, one of the main strengths of this study lies in its pioneering contribution to the analysis of the FAFI as a complementary evaluation tool for joint hypermobility in pediatric populations. The study provides preliminary evidence of the usefulness of this instrument in assessing the foot–ankle complex, an anatomically important yet frequently under-evaluated area. Furthermore, by focusing on a pediatric population, the study addresses a crucial stage for the early detection of biomechanical changes, which may have important clinical implications for prevention and early treatment of dysfunctions.
In conclusion, the study demonstrated a positive, although moderate-to-low, correlation between the Beighton scale and the FAFI. This finding would support the validity of the FAFI as a specific tool for detecting joint hypermobility in the foot–ankle complex. However, further research with larger and more heterogeneous samples is required to strengthen this evidence. The observed concordance also suggests that both tests could be used complementarily, allowing for a more precise clinical evaluation.
Conflicts of interest
None declared
Funding
None declared
Ethics statement
All participants signed informed consent and voluntarily agreed to participate in the study. This study was approved by Universidad de Extremadura Bioethics Committee (Spain) and was planned and conducted in full compliance with the ethical principles outlined in the Declaration of Helsinki. It was approved on March 3rd, 2021, under registration No. 271/2024
Contributions of the authors
Study conception and design: NGL, PCM, BGM.Data collection: NGL, PCM, BGM. Analysis and interpretation of results: NGL, PCM, BGM. Drafting and preparation of the initial manuscript: NGL, PCM, BGM. Final review: NGL, PCM, BGM
References