10.20986/revesppod.2025.1709/2024
ORIGINAL
Comparative study of three techniques for the ring block of the hallux: Frost´s H and modifications
Estudio comparativo de tres técnicas para la anestesia troncular: h de Frost y sus modificaciones
Alicia Ruiz Rivas1
Alfonso Martínez Nova1
1Departamento de Podología. Universidad de Extremadura. Plasencia, Cáceres, España
Abstract
Introduction: In Podiatry, one of the most used anesthetic technique used digitally is Frost´s H technique. However, there are professionals who claim that the lateralization of the needle under the extensor tendon could damage it. Therefore, the aim of this study was to compare the traditional technique with 2 of its variants that do not include lateralization (sweeping technique and 4-point technique).
Patients and methods: The sample consisted of 18 participants, ranging in age from 20 to 27 years. The anesthetic technique was applied randomly, noting the pain experienced during and 10 minutes after the puncture, as well as observing the possible adverse effects 48 hours after the procedure.
Results: After conducting the study, the results obtained were that pain during puncture was 4.2 + 2.2 in the Frost´s H technique, 3.8 + 1.4 in the 4-point technique, and 4.1 + 0.8 in the sweep technique, with no significant differences between them (p = 0.912). Likewise, the effectiveness was similar in the 3 techniques (p = 0.597). The most common complication was posterior hematoma, with no significant differences between groups (p = 0.574).
Discussion: With the results obtained, it is determined that the lateralization of the Frost´s H technique is not harmful to the hallux extensor tendon, as well as that the 3 anesthetic techniques are similar in terms of pain, latency time and efficacy.
Keywords: Digital ring anesthesia, local anesthesia, Frost technique, mepivacaine, nail surgery, foot
Resumen
Introducción: En Podología, una de las técnicas anestésicas más empleada a nivel digital es la H de Frost. Sin embargo, hay profesionales que afirman que la lateralización de la aguja por debajo del tendón extensor podría provocar daños en el mismo. Por ello, el objetivo de este estudio fue comparar la técnica tradicional con 2 de sus variantes que no incluyen la lateralización (técnica de barrido y técnica de 4 puntos).
Pacientes y métodos: La muestra se compuso de 18 participantes, comprendidos en un rango de edad entre 20 y 27 años. Se aplicó al azar la técnica anestésica, anotando el dolor experimentado durante y 10 min tras la punción, así como observando los posibles efectos adversos 48 h después del procedimiento.
Resultados: Tras realizar el estudio, los resultados obtenidos fueron que el dolor durante la punción fue de 4.2 + 2.2 en la técnica en H de Frost, de 3.8 + 1.4 en la de 4 puntos, y de 4.1 + 0.8 en la de barrido, sin existir diferencias significativas entre ellas (p = 0.912). Asimismo, la efectividad resultó similar en las 3 técnicas (p = 0.597). La complicación más común fue el hematoma posterior, sin diferencias significativas entre grupos (p = 0.574).
Discusión: Con los resultados obtenidos, se determina que la lateralización de la técnica en H de Frost no resulta perjudicial para el tendón del extensor del hallux, así como que las 3 técnicas anestésicas presentan similitud en cuanto a dolor, tiempo de latencia y eficacia.
Palabras clave: Anestesia troncular, anestesia local, técnica de Frost, mepivacaína, cirugía ungueal, pie
Corresponding author
Alfonso Martínez Nova
podoalf@unex.es
Received: 04-10-2024
Accepted: 12-02-2025
Introduction
The Frost H anesthetic technique for the first toe is the most widely used method during surgical procedures(1), particularly in nail surgery. These procedures require nerve block of the entire toe, necessitating between 2 a mL nd 4 mL of anesthetic to achieve the desired effect(2). This technique involves a variation of local anesthesia³, which results in reversible and temporary numbness of the area, caused by the temporary inhibition of nerve fiber excitation(4). Among its advantages, this technique, through the infiltration of 2% mepivacaine, allows for toe block throughout the surgical process and provides postoperative analgesia for 1 to 2 hours, facilitating the post-surgical process(5).
The Frost H technique involves two dorsal punctures, one in the lateral region accompanied by lateralization, and another in the medial region?. During the ascending path, anesthetic wheals are left to cover the course of the digital, dorsal, and plantar nerves. The needle also passes under the extensor tendon of the Hallux to anesthetize the dorsal nerves. Typically, this anesthetic procedure does not pose significant risks to the patient?, although some professionals suggest that the lateralization performed may lead to paresthesia, permanent numbness of the area, or damage to the soft dorsal tissues of the first toe. It is also believed that lateralization under the extensor during this procedure could cause damage to the tendon sheath of the extensor complex. However, there is no scientific evidence to support this.
To avoid these potential complications, variations of the technique have been described, such as puncturing the two anatomical points mentioned earlier, omitting lateralization, or the inverted V technique, where infiltration is performed on the dorsum of the first toe, above the extensor tendon, followed by lateralization and infiltration of the lateral and medial regions(5). Other variations involve continuous infiltration during needle withdrawal without aspiration or wheal formation.
Since the efficacy of the Frost H technique compared to its variants (4-point technique, where wheals are left only on the plantar and dorsal parts of each lateral side of the toe, or the sweep technique) is not well understood, and it is unclear whether lateralization under the extensor tendon causes tissue damage, the objective of this study was to evaluate pain during administration, latency time, and adverse effects following infiltration.
Materials and methods
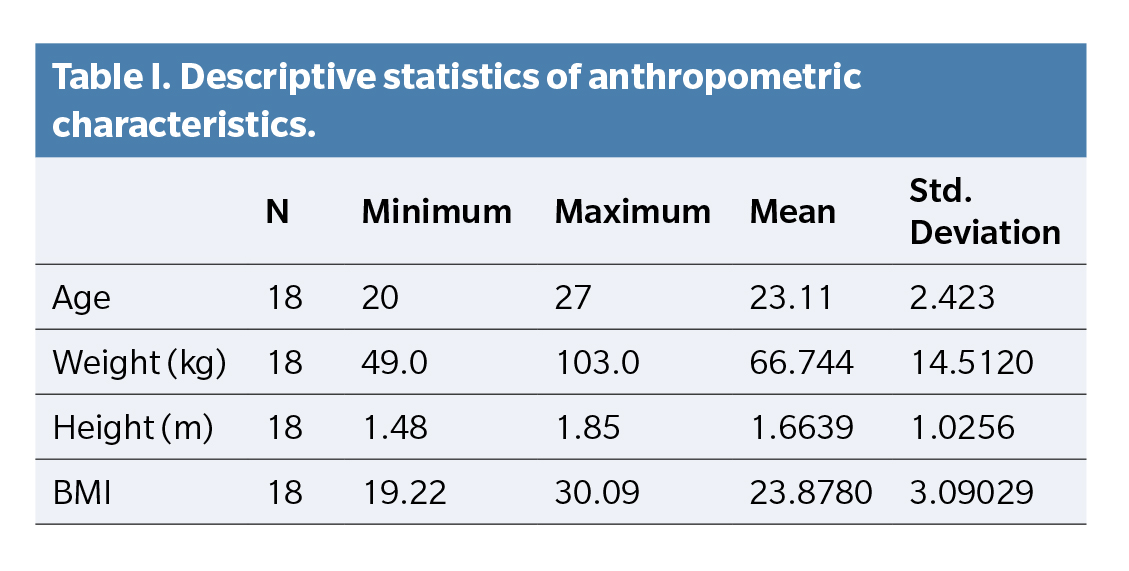
The study consists of a randomized clinical trial that included a total of 18 participants (14 women and 4 men), with a mean age of 23.11 + 2.4 years and a mean weight of 66.7 + 14.5 kg. The minimum and maximum values of these variables are shown in Table 1. All participants volunteered and signed informed consent.
Inclusion and exclusion criteria
Participants meeting the following inclusion criteria were selected: young individuals of both sexes aged between 18 and 30 years, students of Centro Universitario de Plasencia (Spain), those who signed the written informed consent form to participate in the study.
Participants meeting the following criteria were excluded: presence of infection, trypanophobia, allergy to the anesthetic used.
Protocol
After participant acceptance and signing of consent, one of the three anesthetic techniques was randomly applied to each participant, with each group assigned a number:
- Group 1: Frost H (n = 6).
- Group 2: 4-point technique (n = 7).
- Group 3: Sweep technique (n = 5).
The following materials were used for all procedures:
- Sterile drapes.
- Sterile gauze.
- Povidone-iodine.
- 5 mL syringes.
- 27G needles.
- 2 mL of 2% mepivacaine.
Group 1: Frost H anesthetic technique (n = 6)
The Frost H technique (Figures 1 and 2) is a simple process involving two punctures and needle lateralization(4):
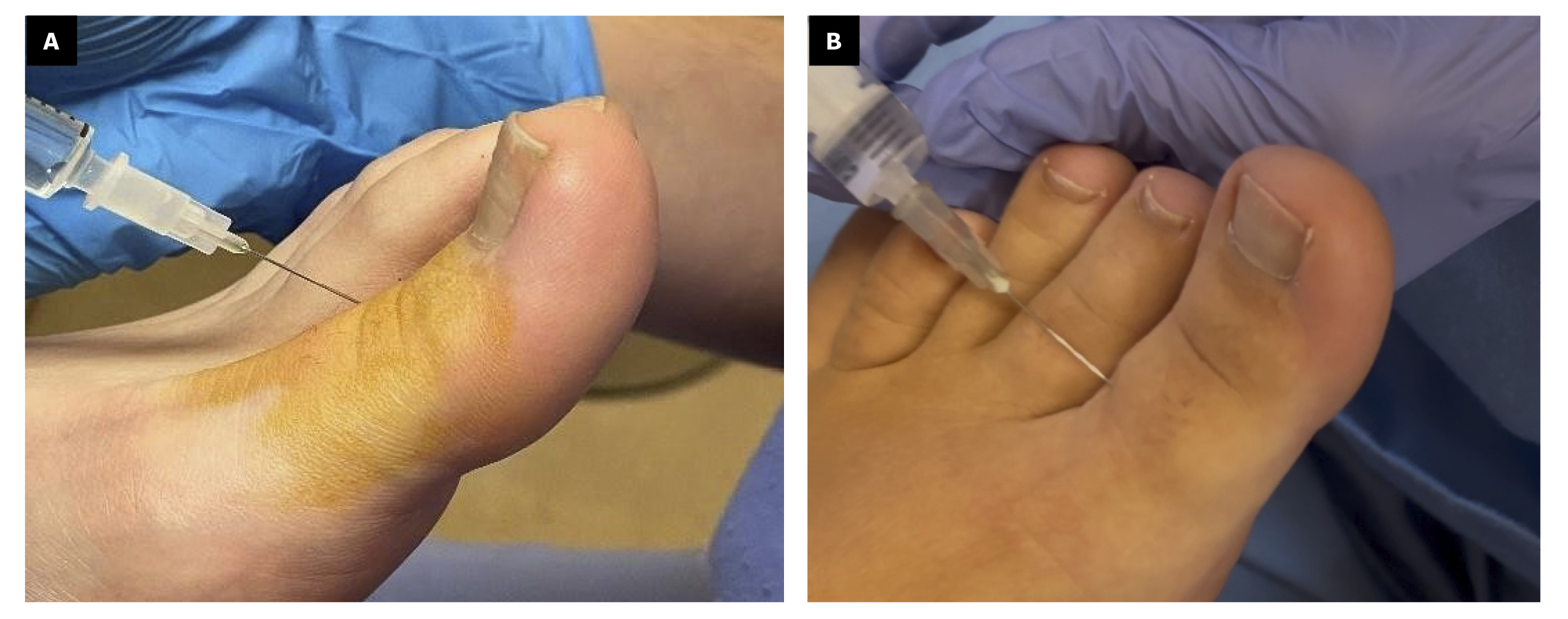
Figure 1. Frost H anesthetic technique. A: First lateral puncture; B: Dorsal lateralization.

Figure 2. Frost H anesthetic.
- First, a puncture is performed in the dorsal and lateral region of the toe, at the start of the interdigital commissure. The needle is inserted until it reaches the plantar region of the toe, taking care not to pierce the skin. Once in this area, aspiration is performed before infiltrating the anesthetic to ensure no capillary has been compromised. If no blood is observed during aspiration, a small amount of anesthetic (approximately 0.15 cc) is infiltrated. The needle is then withdrawn, with aspirations and infiltrations performed along the path until reaching the dorsal region (typically 4 times) (4).
- Afterwards, upon reaching the dorsal region, the needle is not removed. Instead, it is lateralized at 90°, while the toe is dorsiflexed to allow the needle to pass under the extensor tendon of the Hallux. Four more aspirations and infiltrations are performed during the dorsal digital path. The needle is then removed for the second puncture(4).
- Finally, a second puncture is made in the dorsal and medial region of the toe, with aspirations and infiltrations performed similarly during the path(4).
Group 2: 4 point anesthetic technique (n = 7)
- The first step in this technique is a puncture in the dorsal and lateral region, reaching the deep digital level. A first aspiration and infiltration are performed. The needle is then withdrawn to the more superficial level, where a second aspiration and infiltration are performed.
- The needle is removed, and a second puncture is made in the dorsal and medial region, with aspirations and infiltrations performed similarly in the deep and superficial regions. In summary, this technique involves four anesthetic wheals: one deep and one superficial in each respective puncture.
Group 3: Sweep anesthetic technique (n = 5)
This technique is similar to the Frost H technique, with the only difference being the omission of lateralization during the first puncture.
- First, a puncture is performed in the dorsal and lateral region of the toe, reaching the deep level without piercing the skin. Aspirations and anesthetic infiltrations are performed until reaching the surface, ensuring no blood appears during aspirations. Approximately 0.15 cc of anesthetic is administered during each infiltration, typically repeated four times until reaching the dorsal region.
- The needle is then removed, and a second puncture is made in the dorsal and medial region, following the same procedure as in the lateral region. Aspirations and infiltrations are performed, leaving anesthetic along the path of the entire toe until reaching the plantar region.
Measurements
VAS pain scale
After performing the corresponding anesthetic technique, pain resulting from the procedure was assessed using the VAS scale on an iPad (Figure 3). The subject rated the discomfort during the procedure twice, with the value obtained kept hidden to avoid influencing the participant during the second measurement. The average of the 2 values was taken as the definitive pain estimate.
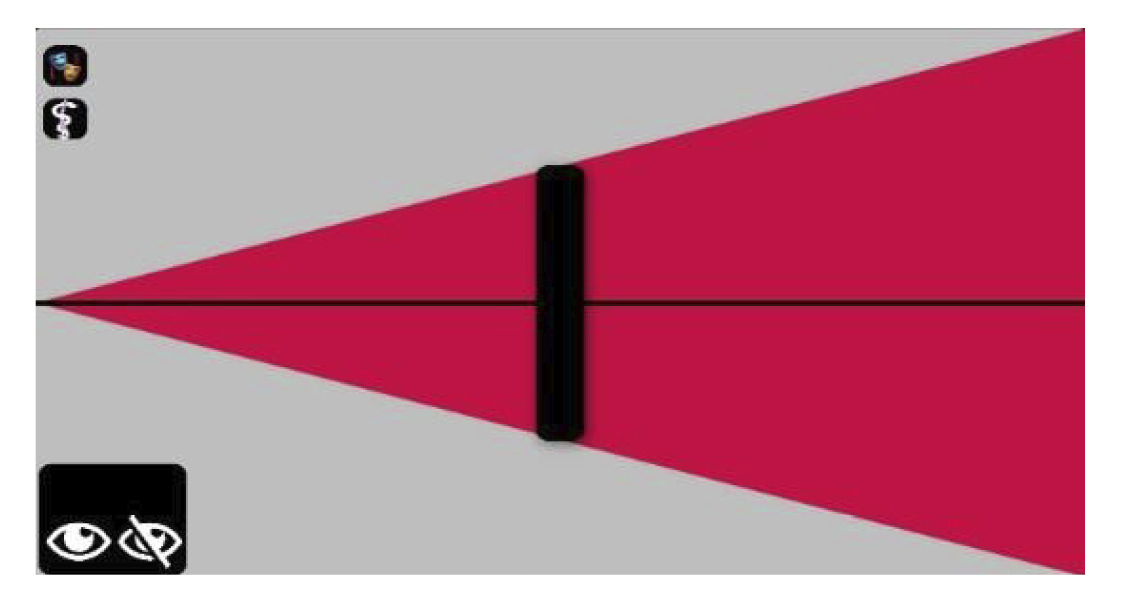
Figure 3. VAS scale with hidden value.
Pain after latency time
Ten minutes after the procedure (mepivacaine latency time?), the anesthetic efficacy was assessed. First, a superficial puncture was made on the pulp of the first toe using a 29G lancet (Figure 4). Sensitivity in the lateral and medial regions of the toe was then checked by vigorously pulling the skin of both regions using Adson forceps. The participant was asked to rate the pain associated with these actions using the iPad VAS scale (2 measurements).

Figura 4. Posterior lancet puncture 29 G.
Assessment of tissue damage and possible complications
Two days after the anesthetic infiltration, other aspects were assessed, both through visual inspection and ultrasound imaging, including: 1) inflammation of the area, 2) redness, 3) presence of hematoma, 4) pain, 5) difficulty or inability to mobilize the first toe, or 6) positive signal in Doppler PwC (ultrasound).
Statistical analysis
We conducted a descriptive analysis of anthropometric variables (mean and standard deviation). To compare the mean pain between men and women, an independent samples t-test was used. To compare pain among the 3 techniques, a one-way ANOVA was applied. Contingency tables and Chi-square tests were used to analyze the relationship between technique and complications. Statistical analysis was performed using SPSS 29 software (IBM SPSS Statistics, UEX license). A p-value < 0.05 was considered significant.
Results
Pain during the procedure
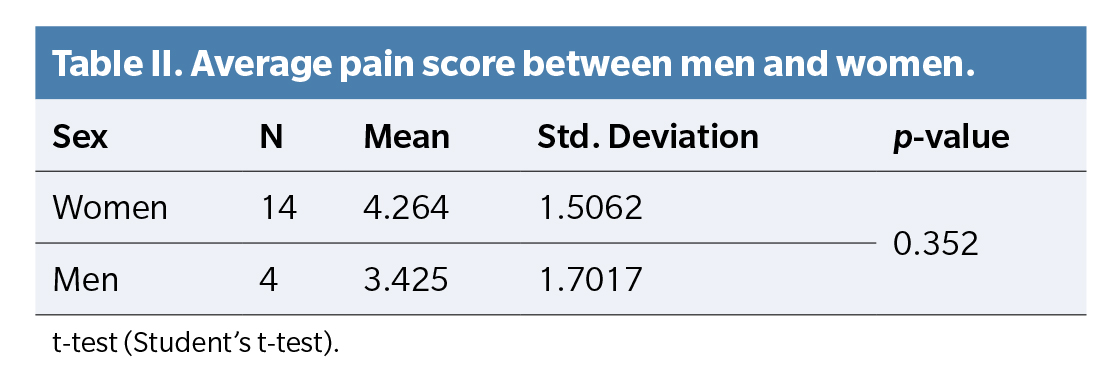
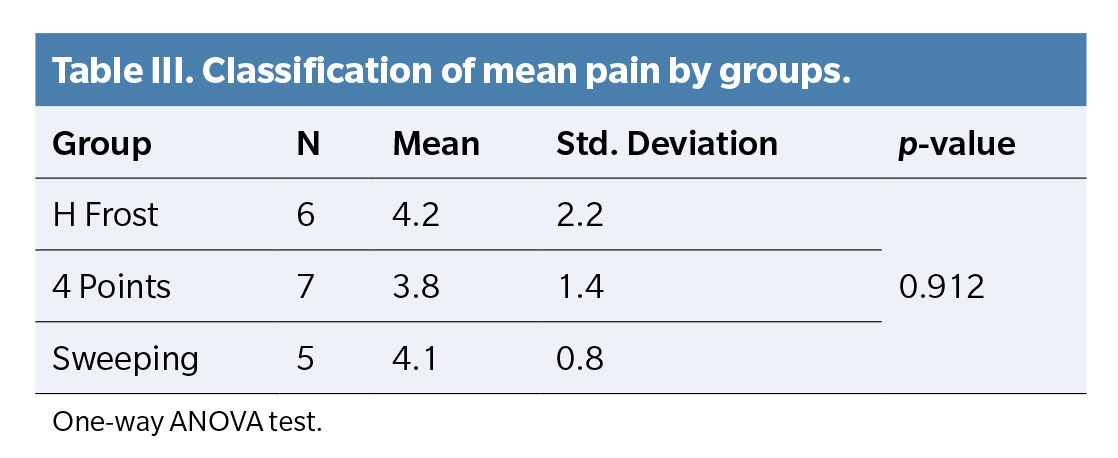
In the overall group, the mean pain in women was 4.3 + 1.5, while in men it was 3.4 + 1.7, with no significant difference between the groups (p = 0.352, Table 2). Regarding mean pain by group, in the Frost H group it was 4.2 + 2.2, in the 4-point group it was 3.8 + 1.4, and in the sweep technique group it was 4.1 + 0.8. There were no significant differences between groups (p = 0.912, Table 3).
Pain after the techniques
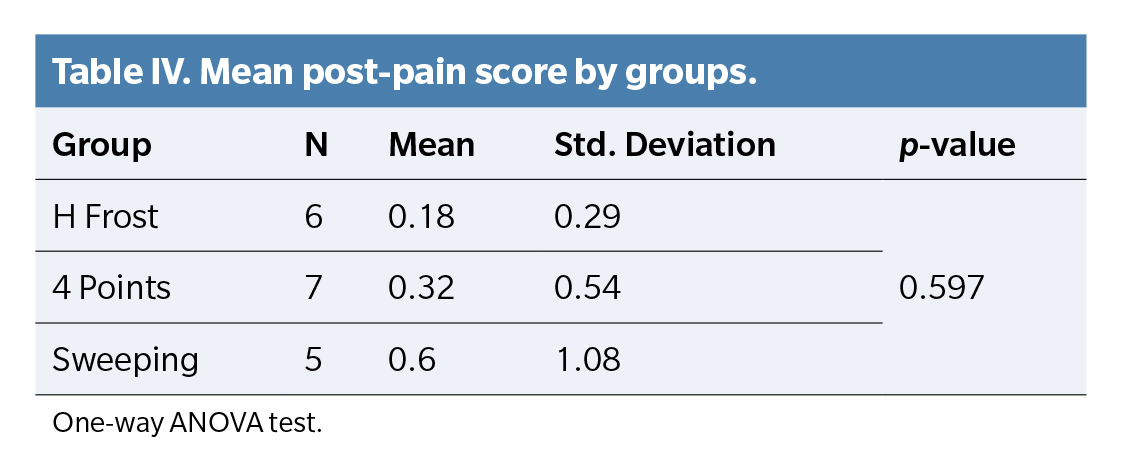
The mean pain in the overall group was 0.35 + 0.65. The mean post-procedure pain in the Frost H technique was 0.18 + 0.29, in the 4-point technique it was 0.32 + 0.54, and in the sweep technique it was 0.6 + 1.08. There were no significant differences in pain between groups (p = 0.597, Table 4).
Complications
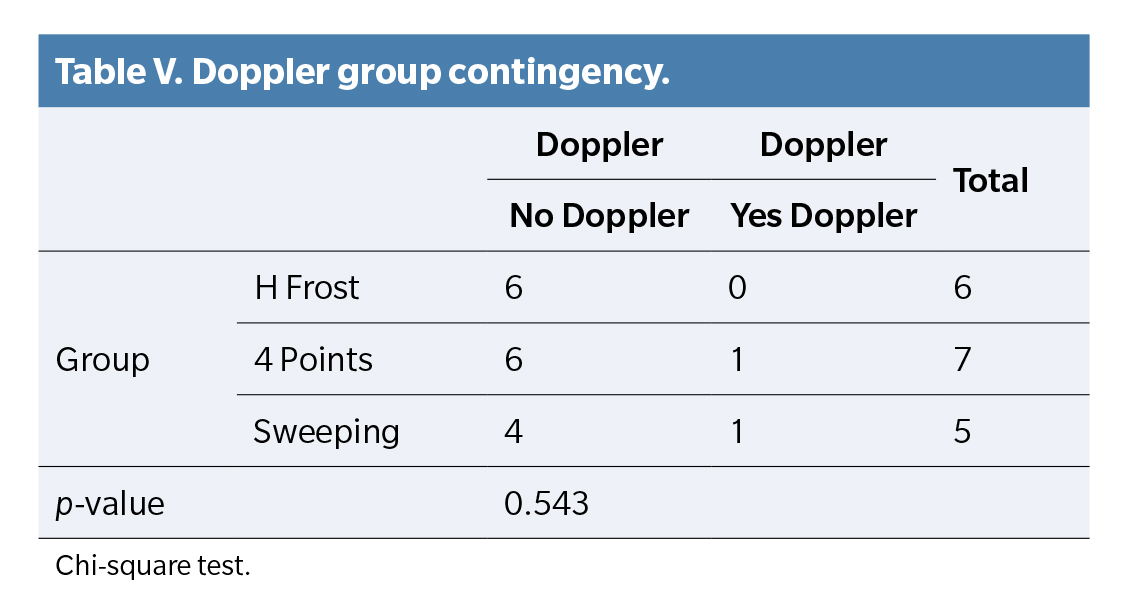
Angiogenesis in Doppler imaging. During ultrasound imaging at 48 hours, structural changes were observed in 2 participants: one from the 4-point technique group and the other from the sweep technique group. The rest showed no structural changes in the ultrasound examination. Differences across groups were not significant (p = 0.543, Table 5).
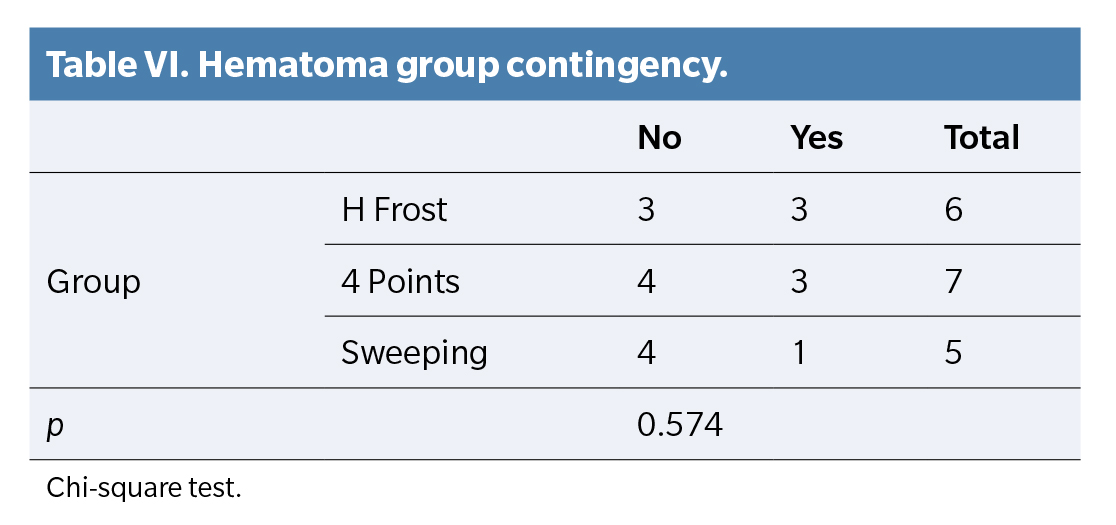
Presence of hematoma. Hematoma was observed in 7 subjects, with 3 from the Frost H group, 3 from the 4-point technique group, and 1 from the sweep technique group. There were no significant differences between groups (p = 0.573, Table 6).
Discussion
Our sample, composed of young participants, showed a mean pain related to the procedure of around 3.8 (Table 2), regardless of the group. This indicates that the pain from anesthetic infiltration is moderate, albeit for a very short period, according to the categorical scale classification(8). Although some studies suggest that women have a lower pain threshold?¹?, this was not demonstrated in our case, as both men and women responded similarly (Table 2). This mean pain is similar to that of other studies, such as one comparing the metatarsal technique with the Frost H technique(11), or another applying the inverted V anesthetic technique for digital block?. Thus, the pain would be caused by the procedure itself, anxiety, tissue distension, the pH of the anesthetic, or its temperature(12), being independent of the technique used. One study indicates that the speed of anesthetic administration influences the perceived pain during the procedure, with faster administration generally being more favorable, although this depends on the individual(13). In this study, all procedures were performed by the same person, so we believe this factor did not significantly influence the results.
Pain experienced after the latency time (10 minutes) was similar for all 3 anesthetic techniques. Thus, variations in the widely used technique do not affect time until the anesthetic effect begins or its efficacy. In this study, 2 cc of 2% mepivacaine was used, which may be sufficient for toe anesthesia. Some participants may have required a larger amount for effective anesthesia due to their size or weight.
Regarding the complications found, the most common one was the appearance of hematoma at the anesthetic puncture site. However, this is common after any puncture due to the rupture of blood vessels that may occur during needle insertion, as well as anatomical variations in each individual, which may predispose them to this complication(14,15).
On the other hand, it is important to note that this complication was reported by study participants in the first few days after the puncture, eventually disappearing without causing any other tissue or structural damage to the toe.
Ultrasound imaging at 2 days did not show quantifiable damage to the extensor complex of the Hallux (Table 6), which was one of the clinical concerns discouraging the use of the Frost H technique. Therefore, it is determined that the possible complications that may have arisen in the study are independent of the technique used in each case.
In conclusion, based on the results obtained in this study, the 3 techniques used (Frost H, sweep technique, and 4-point technique) are similar in achieving their primary endpoint: effectiveness in anesthetic block. Additionally, it is determined that the traditional technique (Frost H) does not present disadvantages compared to the other two techniques, as no tissue damage was observed during the lateralization associated with this technique. Therefore, according to the study findings, any of these three techniques could be used for anesthetic block of the first toe in podiatry, depending on the professional’s preference and criteria. In the authors’ opinion, and based on the results, the 3 techniques would yield satisfactory results for achieving digital numbness; however, the Frost H technique would be the primary choice, reserving the 4-point and sweep techniques for special cases, such as patients with greater difficulty during anesthetic administration, and in children, for the same reason mentioned above.
Regarding the study limitations, the main one was the small sample size, which limits the generalizability of the results. Additionally, the study was conducted on a group of young participants without nail pathology, which may bias the results, as it is unknown whether complete toe anesthesia would have been achieved in a real surgical procedure.
In conclusion, considering the results obtained, the 3 techniques were comparable in terms of pain during the infiltration process, regardless of whether lateralization under the extensor or infiltration by wheals or sweep was performed. Truncal anesthesia of the first toe was effectively achieved with all three variants, with no significant advantage of one over the others. The only complication observed was the appearance of hematoma, considered a normal effect due to needle manipulation along the lateral sides of the toe, unrelated to the technique used.
Ethics Declaration
The present sud tudy was conducted with the approval of the Bioethics and Biosafety Committee of Universidad de Extremadura (Spain) (permission No.: 185//2023).
Authors’ contributions
Study conception and design: AMN.
Data collection: ARR.
Analysis and interpretation of results: AMN.
Drafting, writing, and preparation of the manuscript: ARR.
Final review: ARR.
Conflict of interest
None.
Funding
None.
References
- Martínez Nova A. Podología. Atlas de Cirugía Ungueal. Madrid: Ed. Médica Panamericana; 2006.
- Sánchez Hernández S, Giralt de Veciana E. Comparación de 2 técnicas de bloqueo anestésico en el tratamiento quirúrgico de onicocriptosis del primer dedo del pie. Actas Dermosifiliogr. 2022;113:370-5. DOI: 10.1016/j.ad.2021.12.013.
- Acosta-Martínez J, Guerrero-Domínguez R, López-Herrera-Rodríguez D, Sánchez-Carrillo F. Rol del anestesiólogo. Rev Colomb Anestesiol. 2016;44(2):121-7. DOI: 10.1016/j.rca.2016.02.010.
- Martínez Nova A, Córdoba Fernández A, Juárez Jiménez JM, Rayo Rosado R. Monitorización, sedación y técnica anestésica para la cirugía ungueal. En: Martínez Nova. Atlas de Cirugía Ungueal. 2ª ed. Madrid: Panamericana; 2014. p. 59-66.
- Sánchez S, Gordedo Silva M. Estudio observacional de la eficacia del bloqueo anestésico en el primer dedo del pie utilizando la Técnica V Invertida: Un procedimiento innovador. Rev Iberoam Podol. 2024;5(1):E0702023. DOI: 10.36271/iajp.v5i1.70.
- Trepal MJ, Jules KT. Anestésicos locales en cirugía podológica. Rev Int Cie Podol. 2007;1(1):49-74.
- Arribas Blanco J, Rodríguez Pata N, Esteve Arrola B, Beltrán Martín M. Anestesia local y locorregional en cirugía menor. SEMERGEN. 2001 [citado 30 Mar 2024];27(9):471-81. Disponible en: https://www.elsevier.es/es-revista-medicina-familia-semergen-40-articulo-anestesia-local-locorregional-cirugia-menor-13020294 DOI: 10.1016/S1138-3593(01)74380-8.
- Vicente-Herrero MT, Delgado-Bueno S, Bandrés-Moyá F, Ramírez-Iñiguez- de-la-Torre MV, Capdevilla-García L. Valoración del dolor. Revisión comparativa de escalas y cuestionarios. Rev Soc Esp Dol. 2018;25(4):228-36.
- Carneiro de Araújo Palmeira C, Adel Ashmawi H, TSA, de Paula Posso I. Sexo y percepción del dolor y analgesia. Rev Bras Anestesiol. 2011;61(6):449-58.
- Gutiérrez Lombana W, Gutiérrez Vidal SE. Pain and gender differences: A clinical approach. Colomb J Anesthesiol. 2012;40(3):207-12. DOI: 10.1016/j.rcae.2012.05.006.
- Oliva-Martín C, Manuel Jiménez-Cano V, Martínez-Nova A. Estudio comparativo entre dos técnicas de anestesia local troncular del primer dedo. Rev Esp Podol. 2022;33(1):14-25. DOI: 10.20986/revesppod.2022.1605/2021.
- Noël B. Anesthesia for ingrowing toenail surgery. Dermatol Surg. 2010;36(8):1356-7. DOI: 10.1111/j.1524-4725.2010.01640.x.
- Eche Herrera J, Franco Quino C, Chumpitaz Cerrate V, Castro Rodríguez Y. Influencia de la temperatura de la lidocaína 2% con epinefrina 1:80,000 sobre el dolor por inyección e inicio de acción en el bloqueo dentario inferior. Rev ADM. 2015;72(5):236-42.
- Soler E, Faus MT, Burguera R, Fernández JA, Mula P. Anestesiología 2. Madrid; 2005.
- García Peñín A, Guisado Moya B, Montalvo Moreno JJ. Riesgos y complicaciones de anestesia local en la consulta dental: Estado actual. RCOE. 2003;8(1):41-63. DOI: 10.4321/S1138-123X2003000100004.