DOI: http://dx.doi.org/10.20986/revesppod.2024.1683/2023
ORIGINAL
Ganador Premio Virginia Novel 2023
Peroneus longus potentiation in subjects with flexible dorsiflexed first ray. Prelimimary results of a randomized clinical trial
Potenciación del peroneo largo en sujetos con primer radio dorsalflexionado flexible.
Resultados preliminares de un ensayo clínico aleatorizado
Priscila Távara Vidalón1
María José Manfredi Márquez2
1Departamento de Podología. Universidad de Sevilla, España
2Clínica privada. Alcalá de Guadaira, Sevilla, España
Abstract
Objectives: To analyze the changes produced in the plantar pressures of the first ray after an exercise program to strengthen the peroneus longus muscle.
Patients and methods: In 24 subjects with a flexible dorsiflexed first ray, the dorsiflexion and plantarflexion of the first ray, the dorsiflexion of the 1st metatarsophalangeal joint, the strength of peroneus longus, the FPI, and the plantar pressures under first metatarsal head were assessed. The sample was randomly divided into two groups. The experimental group performed exercises to strengthen the peroneus longus with elastic bands for 4 weeks.
Results: In the study group, statistically significant differences were obtained with an increase in plantarflexion of the first ray (p = 0.016); a percentage decrease in first metatarsal head loading time (p = 0.036); and an increase in the percentage of the time interval in which their maximum pressure occurs (p = 0.008). Comparing both groups, significant differences were found in dorsiflexion (p = 0.022) and plantarflexion of the first ray (p = 0.027); and in the maximum pressure value of the entire stance phase (p = 0.031).
Conclusion: The subjects who performed the exercise program with elastic bands to strengthen the peroneus longus after four weeks, presented an increase in the plantarflexion of the first ray, in the first metatarsal head pressure during the stance phase and in its maximum pressure in dynamics.
Keywords: First ray, foot, exercise, Peroneus Longus, dorsiflexion, plantarflexion
Resumen
Objetivos: Comprobar los cambios producidos en las presiones plantares del primer radio tras un programa de ejercicios de fortalecimiento del músculo peroneo largo.
Pacientes y métodos: En 24 sujetos con un primer radio dorsalflexionado flexible, se valoró la dorsalflexión y plantarflexión del primer radio, la extensión de la 1.ª articulación metatarsofalángica, la fuerza del peroneo largo, el FPI, y las presiones plantares de la cabeza del primer metatarsiano en dinámica. La muestra se dividió aleatoriamente en dos grupos. El grupo experimental realizó ejercicios para potenciar el peroneo largo con bandas elásticas durante 4 semanas.
Resultados: En el grupo de estudio se obtuvieron diferencias estadísticamente significativas con un aumento en la plantarflexión del primer radio (p = 0.016), una disminución del porcentaje del tiempo de carga de la cabeza del primer metatarsiano (p = 0.036) y un aumento en el porcentaje del intervalo de tiempo en el que se produce su presión máxima (p = 0.008). Comparando ambos grupos, se encontraron diferencias significativas en la dorsalflexión (p = 0.022) y plantarflexión del primer radio (p = 0.027) y en el valor máximo de presión de toda la fase de apoyo (p = 0.031).
Conclusiones: Los sujetos que realizaron el programa de ejercicios con bandas elásticas para potenciar el peroneo largo tras cuatro semanas presentaron un aumento del rango de movimiento de la plantarflexión del primer radio, de la presión de la cabeza del primer metatarsiano durante la fase de apoyo y de su presión máxima en dinámica.
Palabras clave: Primer radio, pie, ejercicios, peroneo largo, dorsiflexión, plantarflexión
Correspondence: Priscila Távara Vidalón
priscilatavara16@gmail.com
Received: 17-12-2023
Accepted: 18-03-2024
Introduction
The first ray is a functional unit formed by the first metatarsal and the medial cuneiform bone(1), and has an important component in the stability and structural integrity of the foot(1). It plays a fundamental role in the gait cycle, as it results from a balance between the reactive forces of the ground and the support structures that stabilize the medial column of the foot(3).
In the propulsive phase of gait, the first ray must plantarflex so that the first metatarsal head presses firmly on the ground(4). This movement is due to the contraction of the peroneus longus muscle(1,5,6,7) (PL), which works synergistically with the tibialis posterior, generating a compressive force that favors the stability(1,7,8). In this way, the PL plays a significant role in the support and stability of the foot in dynamics9, and together with the windlass mechanism, it allows correct propulsion to develop(8,10).
Because of its anatomy, the PL has a mechanical advantage for plantarflexing the first ray. An alteration in its function can cause the distance of its insertion to approach the plane of the floor, thus decreasing the stability of the foot(4,11), and can cause the tibialis anterior to gradually elevate the first ray(12).This situation of instability is defined as hypermobility of the first ray(4), which will imply biomechanical changes in the foot and will be responsible of pathologies such as metatarsalgia , stress fractures of the second metatarsal, hallux abductus valgus (HAV), flat feet, or plantar fasciitis(3,13,14). Furthermore, dorsiflexion of the first raywill decrease the range of motion of the first metatarsophalangeal joint (1st MTPJ) and may cause hallux limitus or hallux rigidus(1).
There are different types of corrective or compensatory treatments for instability or insufficiency of the first ray, such as surgical and orthopedic. In theory, in those cases in which there is a flexible dorsiflexed first ray, if the action that the PL exerts on the first ray is enhanced, the stability and load capacity will improve. Muscular strength can be improved by performing resistance or strength training(15) , using exercises with elastic bands(15,16,17,18). This has the advantage that the patient could develop it at home, it implies very low risk and does not have any type of side effects. The main drawback would be the lack of consistency and adherence to treatment without the supervision of the clinician.
To our knowledge, there are no studies in the literature that report on whether strengthening the main plantarflexor muscle of the first ray, the PL, contributes to improving its stability and reestablishing its load capacity in the final stance phase of. Therefore, the main objective of this study is to determine whether training through an exercise program with elastic bands in subjects with a flexible dorsiflexed first ray for (4) weeks can improve its function, evaluating the changes produced in both statics and dynamics.
Patients and methods
This study consists of a randomized, controlled clinical trial, which was carried out in accordance with CONSORT recommendations(19).
Participants
The sample of this study was made up of adult subjects who attended the Podiatry Clinical Area of the University of Seville, as long as they met the selection criteria and agreed to participate in the study voluntarily.
This work was carried out between the months of September 2022 and July 2023. The inclusion criterion was: to present flexible dorsiflexed first ray20. The exclusion criteria were: having suffered from trauma that could affect the mobility of the first ray; first ray surgery; present HAV; under going some orthopedic or orthopedic treatment; and/or having suffered systemic, degenerative or neuromuscular diseases that affect the feet.
Data collect
Clinical examination
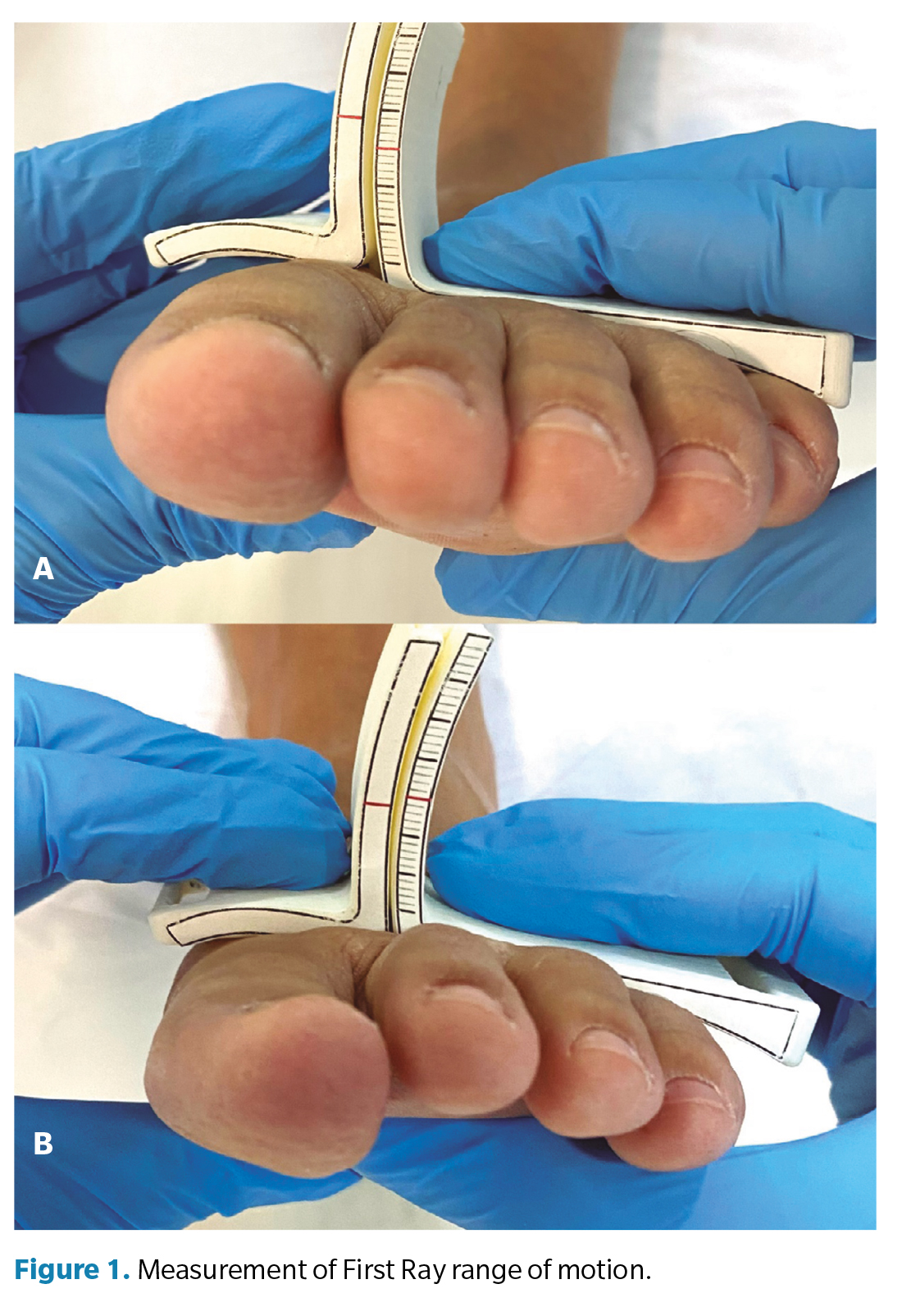
The clinical examination of all subjects was performed by a podiatrist with more than 10 years of experience. First, to determine whether participants had the study condition, i.e., flexible dorsiflexed first ray, maximum dorsiflexion / plantarflexion of the first ray was assessed. To do this, the subject was placed on a examination table in a supine position with the ankle relaxed and the subtalar joint in a neutral position. Afterwards, the mobility of the first ray was measured with a measuring instrument(20) to register the range of motion in millimeters of maximum dorsiflexion , following the protocol previously described in other research works(20,21,22) The head of the first metatarsal was moved upward to its maximum range in dorsiflexion (Figure 1A) and was subsequently moved downward to its maximum range in plantarflexion (Figure 1B). The range of motion was determined by observing on the instrument‘s ruler how many millimeters it moved in both positions.
Subjects who met the inclusion criteria were eligible for the study, and the other parameters were explored. The following protocol was developed:
- First metatarsophalangeal joint dorsiflexion: the hallux was hold together with the distal branch of the goniometer towards maximum extension, allowing the first ray to plantarflex so that the extension movement occurred completely(1).
- Foot PostureIndex (FPI): FPI was measured following the protocol described by Redmond et al.23 with which a score would be obtained for each foot. Normal values are set in the range from 0 to +5.
- Force exerted by the first metatarsal: a specific muscle examination of the PL was performed with a dynamometer (ActivForce® 2 Digital. Activbody. San Diego CA, USA) to quantify the force in Newtons. With the participant in a supine position, performing eversion and plantar flexion of the foot, they had to press the active surface of the dynamometer with the head of the first metatarsal while the researcher exerted resistance.
- Plantar pressure of the first ray: the plantar pressures of the first ray were measured using Footscan(9) (RsScanLab, Ltd. United Kingdom) 43 cm wide by 205 cm long. A dynamic analysis was performed, in which the subject was placed standing on the ground in a straight forward line. They were instructed to take a few steps on the platform in order to normalize their walking pattern and then the footprints were recorded. Five steps were recorded24.25 with the study foot. The purpose of this step was to record and compare the maximum pressure under the head of the first metatarsal. We chose the 3 most representative footprints, discarding the first one and the last one, the following variables were registered using the mean data of the 3 selected footprints: the average value of the pressure of the first metatarsal head during the stance phase of gait (N/cm2); the percentage of loading time of the first metatarsal head during the stance phase of gait; the maximum pressure value of the whole stance phase (N/cm2); and the percentage of the time interval in which this maximum pressure occurred during the stance phase.
Group training and randomization
The sample was randomly divided into two groups: experimental or study group and control group. The study group consisted of subjects who completed the training program. And the control group wasmade up of subjects who did not perform any type of exercise.
To perform the randomization, the Excel macro AleatorMetod.xls was used, freely available at www4.ujaen.es/~mramos/EPIP/AleatorMetod.xls.
PL strengthening program
The intervention for the experimental group consisted of performing a series of exercises with elastic bands to strengthen the PL muscle, based on the rehabilitation program described by Cain et al.26 in 2020, which consisted of performing exercises of 3 sets of 10 repetitions, 3 times a week for 4 weeks.
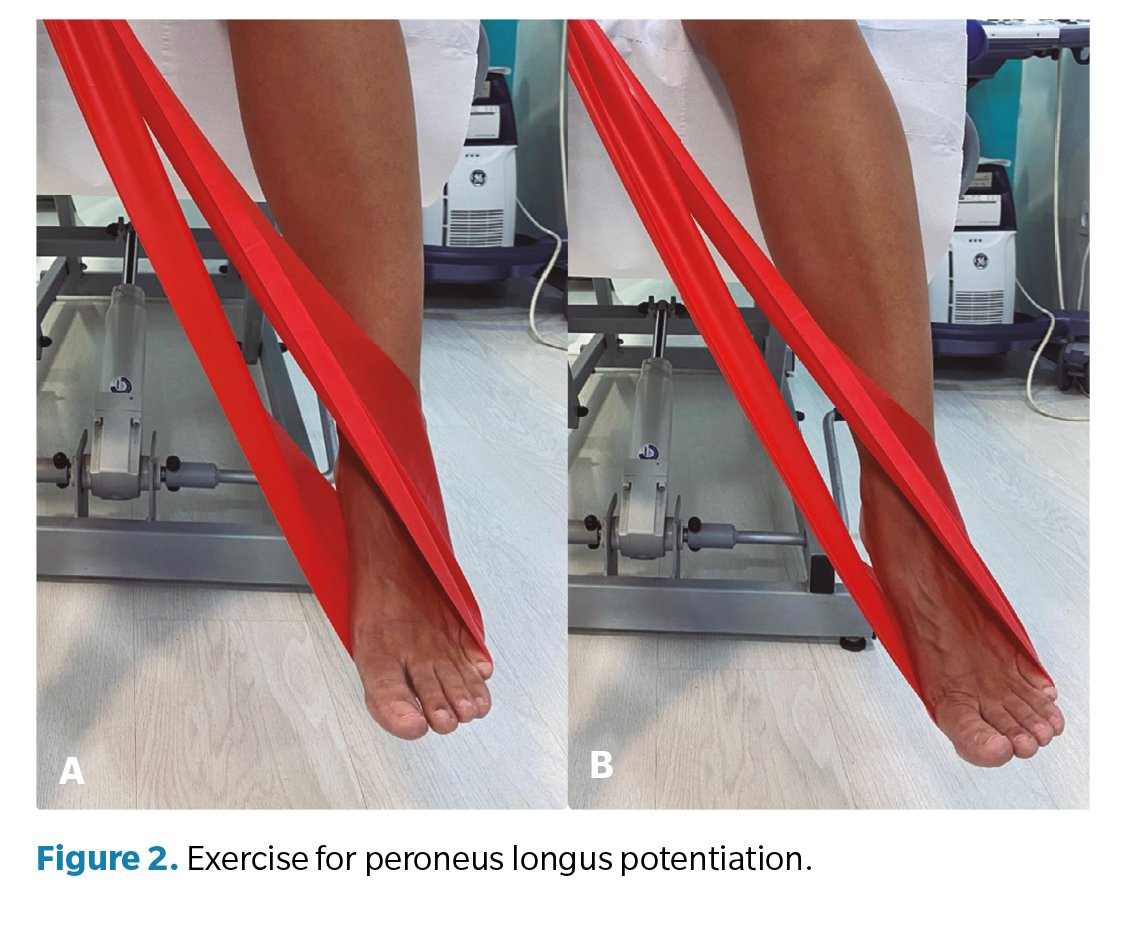
To perform this, the subject was placed in a sitting position with the knees flexed at 90degrees. The band was placed on the study foot and its two ends were held by one hand to generate slight tension (Figure 2A). From here, they performed the eversion movement of the foot with depression of the first metatarsal head and slight plantar flexion (Figure 2B).
During the follow-upperiod, to control that the exercises were carried out, the study group participants were phone contacted to remind them to do the exercises.
Data analysis
The statistical analysis of the data was carried out using the IBM® SPSS®Statistics program (IBM, Armonk, NY, USA). As descriptive data, the absolute frequency (N), relative frequency (%), mean values, standard deviation, median and interquartile range were provided. Normality tests were used to determine whether the data followed a normal distribution, and to know if comparisons should be made using parametric tests (Student ‘s t test for independent samples for inter-group comparisons, and Student ‘s T test for related samples). for pre-post intra -group comparisons) or non-parametric (Mann-Whitney U test for inter-group comparisons, and Wilcoxon test for pre-post intra -group comparisons). The Chi square test was used for comparisons of categorical variables in the previous exploratory analysis. p-values lowerthan 0.05 was considered statistically significant. To determine the magnitude of the statistically significant differences, the effect size was calculated. This was obtained from the Cohen d. Effect size was considered low when it was less than or equal to 0,2, moderate when it was from 0,3 to 0,8, and large when it was greater than 0,827.
Results
The sample for this study consisted of 32 feet of 24 subjects, 16 inthe study group and 16 in the control group. Twenty-one left feet and 11 right feet were included. The distribution by laterality between the two groups wasnot significant (p = 0.063). In the study group, 9 were men and 7 were women. In the control group, 8 were men and 8 were women. The sex distribution was not statistically significant between the two groups (p = 0.956). The age in the study group was 23.44 ± 1.15 years (range 21-25) and in the control group it was 23.56 ± 1.63 years (range 21-27) (p = 0.956). The BMI in the study group was 22.44 ± 2.89 (normal weight) and in the control group was 23.52 ± 2.81 (normal weight) (p = 0.293).
Intraobserver reliability was determined in a previous study(28) in which one of the authors(PTV) measured dorsiflexion and plantarflexion of the first ray using the aforementioned measuring instrument twice in 24 subjects with a separation period between 10 and 30 days between measurements. The intraclass correlation coefficient was calculated (two-factor mixed model) and the results suggested that the reproducibility of the measurement procedure was good(29) (ICC = 0.885 in dorsiflexion; ICC = 0.884 in plantarflexion).
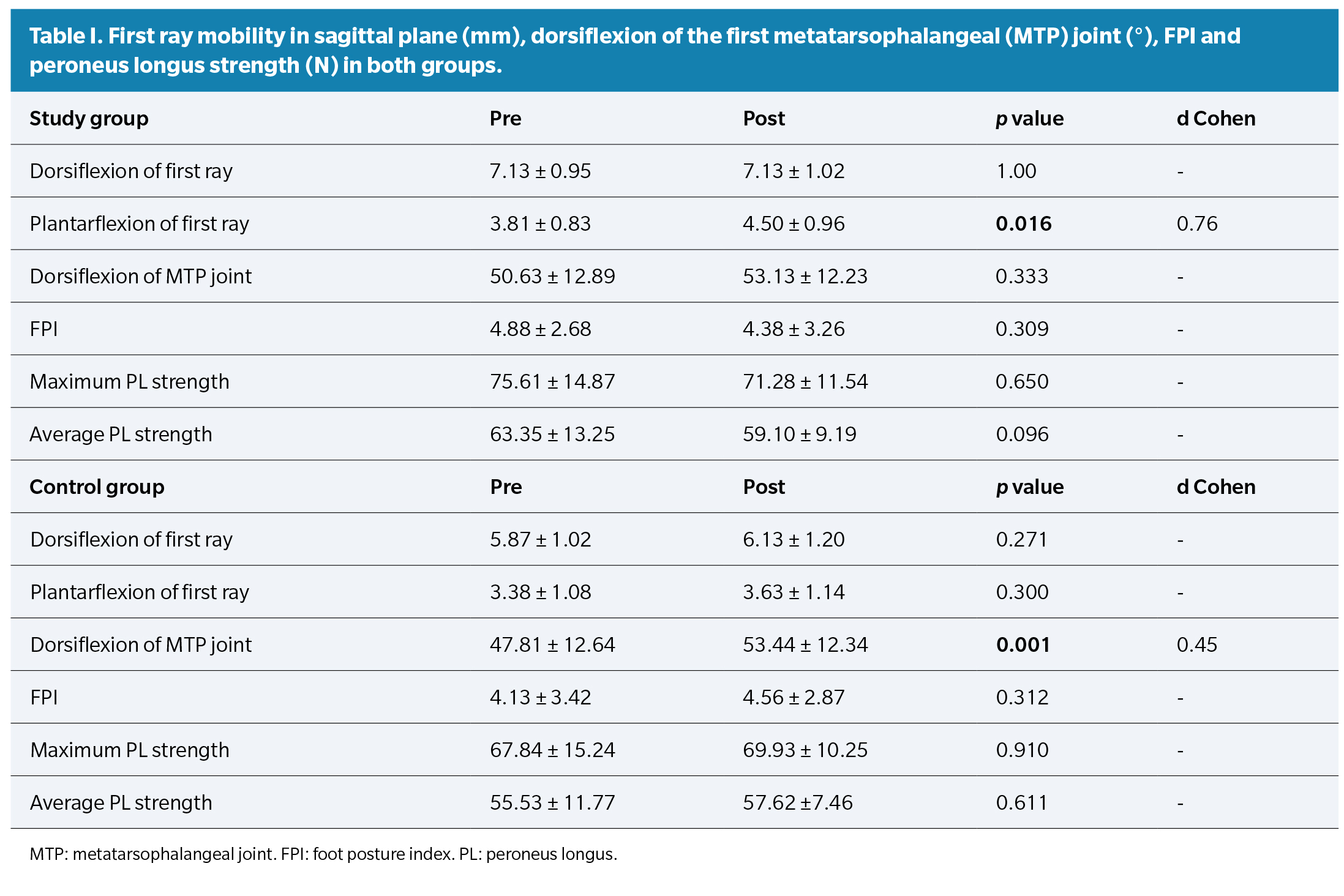
Dorsiflexion and plantarflexion of the first ray; the total movement of halluxextension; The FPI and PL strength measured with the dynamometer in both groups are shown in Table 1. We compared the variables before and after the follow-up periodwithin each group. In the study group, statistically significant differences were obtained in plantarflexion of the first ray (p = 0.016) in which we observed an increase in the range of motion from 3.81 mm to 4.50 mm. In the control group, significant differences were obtained in hallux extension in which the value increased from 47.81° to 53.44° (p = 0.001).
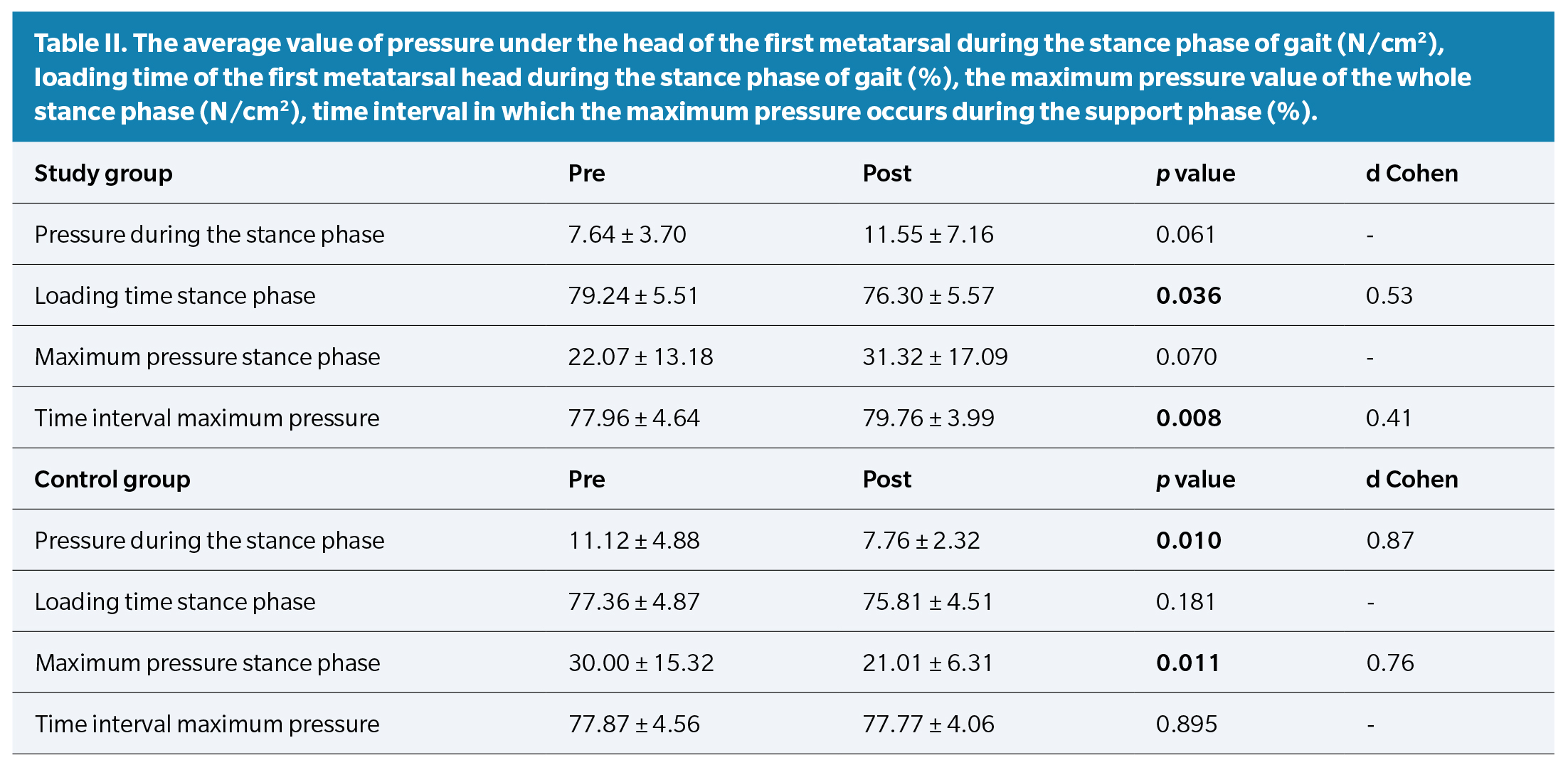
Plantar pressure variablesare shown in Table 2. We compared the variables before and after the follow-up periodwithin each group. In the study group, we obtained significant differences in the variables of the percentage of loading time of the first metatarsal head during the stance phase of gait (p = 0.036), in which a decrease from 79.24 to 76.30 % was observed; and in the variable percentage of the time interval in which this maximum pressure occurs during the support phase (p = 0.008), in which an increase from 77.96 to 79.76 % was observed. In the variables of the average value of pressure under the head of the first metatarsal during the stance phase of gait and the maximum pressure value of the wholestance phase, we did not obtain significant differences (p = 0.061 and 0.070 respectively), but We did observe an increase in pressure under the head of the first metatarsal after carrying out the PL exercise program (pressure in the stancephase: from 7.64 to 11.55 N/cm2 and maximum pressure: from 22.07 to 31 .32 N/cm2). As for the control group, significant differences were obtained both in the average value of pressure underthe first metatarsal head during the stance phase (p = 0.010) and in its maximum pressure (p = 0.011), but in both cases, the variables have decreased their value.
Finally, we compared the variables obtained before and after the follow-up period between groups. The comparison of the dorsiflexion of the first ray and maximum pressure value of the whole stancephase already showed significant differences before starting the strengthening program (p = 0.002 and p = 0.026 respectively). After 4 weeks of exercises, significant differences were also found in dorsiflexion of the first ray (p = 0.022); in plantarflexion of the first ray, in which the value of the study group was 4.50 mm compared to 3.63 mm of the control group (p = 0.027); and in the maximum pressure value of the whole stancephase in which the value of the study group was 31.32 N/cm2 compared to 21.01 N/cm2 of the control group (p = 0.031).
Discussion
The main objective of this investigation was to determine whether PL training using an elastic band exercise program for 4 weeks can improve first ray function in subjects with a flexible dorsiflexed first ray. To do this, we carried out a pre and post comparison of different variables measured in a non-weight bearing position and during gaitwith the use of a pressure platform.
The results indicate that the plantarflexion of the first ray improved, and as a result, the load-bearing functionof the first ray in the stance phase. We think that this increase in plantarflexion of the first ray, as well as the increase in pressure of the head of the first metatarsal during gait, may be due to the fact that these exercises performed with elastic bands helped to enhance the PL and that it exerts a plantarflexor effect of the first ray that can contribute to increase this movement and, consequently, to increasethe pressureunder the first metatarsal head in the stance phase of gait (30,31).
Regarding the methodology selected for this study, we opted for exercises with elastic bands. Although there are no studies that demonstrate effectiveness in the peroneus longus muscle, some authors obtained good results when used to strengthen other muscles and to improve ankle stability(15,16,18,26,32)..
In regard to other types of exercises to increase PL activity, Bavdek et al.(33) evaluated the muscular activity of the PL and PC using electromyography, during gaiton different surfaces. Their results showed greater activation of the peroneal muscles when walking on a 30° inclined ramp compared to a flat surface. These authors suggest that walking on an inclined surface may be a useful type of exercise to strengthen the peroneal muscles. Although they obtained good results in isometric muscle contractions, walking on an inclined surface can cause injuries if the inversion angle exceeds 35° degrees(34). Additionally, one of the limitations of this study was that after performing several steps, muscle habituation occurred that led to a decrease in its activity over time, making this activity less effective in strengthening muscles. For this reason, we believe that opting to strengthen the PL with elastic bands can be more effective when it comes to strengthening this muscle.
Regarding the results obtained, the plantarflexion of the first ray increased and also its load function during the stance phase of gait, showed improvement. Regarding this, Dullaert et al.(10) carried out a study with 8 cadaver legs in which CT images were taken in a neutral position without load (75 N), with load (700 N) and with 15 kg weights hanging from the PL tendon, simulating its contraction. One of the measurements they calculated was the Meary angle, whose normal value is less than 10° degrees. Their results indicated that this angle increased with loading from 75 to 700N (from 6.84° degrees to 9.16° degrees; p > 0.01). This could be transferred to our study in that just by standing up, the first metatarsal decreases its verticality and therefore its plantarflexion. This may be a possible explanation for the fact that we only obtained significant differences in the unloading measurements with an increase in plantarflexion of the first ray, despite the fact that the loading measurements were also increased when the PL was enhanced. Furthermore, in this study the results were obtained that when applying a 15kg load to the PL tendon there was also an increase in the Meary angle from 9.16° to 10.45°; p = 0.52). Although the increase was small, what was expected was that the PL traction would decrease this angle. We think that, unlike our study, performing an in vitro studymay be a disadvantage compared to performing it in vivo,sincemuscles can be trained and their power increased following a training plan, as demonstrated by other studies that use elastic bandsto strengthen the muscles of the upper and lower limbs(15,16,18,26,35,36,37,38,39).
On the other hand, we obtained significant differences in the variables of the percentage of loading time of the first metatarsal head during the stance phase of gait (p = 0.036), in which a decrease was observed; and in the variable percentage of the time interval in which this maximum pressure occurs during the stancephase (p = 0.008), in which an increase was observed. We believe that this may be because performing the exercises and strengthening the PL helps improve the functionality of the first ray. This is why a decrease in the loading period of the metatarsal during the stance phase has been observed (from 79.24 to 76.30 %) since, if the first ray is dorsiflexed, it is possible that this time is longer because at the same time Pronating the foot shifts ground reaction forces toward the medial forefoot for longer periods of time.
The time interval in which this maximum pressure occurs, increased. We think this is because with the strengthening of the muscle and its improvement in the loading of the first ray, it is possible that it began to load less time in the support phase because it began to load later and more efficiently. Hence, the moment in which the maximum load occurred was closer to takeoff after the monitoring period (from 77.96 % to 79.76 %).
Regarding the comparative analysis at the beginning and at the end of the follow-up, in the control group only statistically significant differences were obtained in the metatarsophalangeal dorsiflexion, in which, although an increase from 47.81 to 53.44° was observed, We think that this difference of 5.6° is low, because this measurement is obtained with the two-branch goniometer and the values are marked each 10 degreesand therefore does not present clinical significance.
Regarding the variables measured with the pressure platform, the control group obtained significant differences both in the average value of the pressure of the first metatarsal head during the stance phase (p = 0.010) and in its maximum pressure (p = 0.011). But, in both cases the variables have decreased in value. We think that the possible explanation for this inconsistency in the results may be due to the small sample size used in this pilot study, since these subjects did not undergo any type of treatment that could influence this change.
Finally, we compared all the variables at the end of the 4 weeks between both groups. The results show that there were significant differences in the dorsiflexion of the first ray (p = 0.022), in which the value of the study group was 7.13 mm compared to 6.13 mm of the control group; in plantarflexion of the first ray (p = 0.027), in which the value of the study group was 4.50 mm compared to 3.63 mm of the control group; and in the maximum pressure value of the whole stancephase (p = 0.031), in which the value of the study group was 31.32 N/cm2 compared to 21.01 N/cm2 of the control group. Regarding dorsiflexion, although the results were statistically significant, we do not consider them relevant, since at the beginning of the study significant differences were also found (p = 0.002). These results should be interpreted with caution, since we consider that an increase in the sample size would homogenize the groups, in terms of this variable.
On the other hand, regarding plantarflexion and maximum pressure of the first metatarsal, the study group obtained a higher value compared to the values of the control groupafter 4 weeks of training, presenting significant differences. We think that this may be because this exercise program may have contributed to the improvement in the functionality of the first ray both in its assessment of discharge and dynamics.
Previous studies evaluatedthe influence of conservative elements on PL activity. Ludwing et al.(40) studied the increase in PL activity with the use of a lateral pressure element placed in a personalized orthopedic insole. Thirty-four healthy subjects participated and walked down a catwalk using the same model of footwear. In addition, two types of orthopedic insoles were used, one standard and the other sensorimotor (standard insole to which a 35 shoreA piece of EVA was added to the lateral edge of the rearfoot in order to stimulate the area). Contact with the ground was recorded through two pressure sensors under the sole of the shoe. Their results indicated that an increase in PL activity occurred during the propulsive phase and the mid-support phase when sensorimotor insoles were used. Furthermore, they considered that the pressure point changes the afferent information and leads to greater activation of the PL in the time interval in which the pressure point exerts pressure on the peroneal tendon.
Roca-Dols et al.(9) assessed the activity of the PL and peroneus brevis in healthy subjects, walking in 6 different situations, with the participants barefoot and with the participants wearing 5 different types of footwear. Their results indicated that, during the propulsive phase of walking, the PL reduced its activity in cases in which the subjects were wearing shoes with an air chamber compared to walking barefoot. The authors consider that the cushioning mechanism of the shoe could reduce PL activity in this phase. However, during the contact phase, footwear with an air chamber increased the activity of the PL, and this may be due to the cushioning mechanism of the sole, which provides lateral stability. In short, they consider that the result of muscular activity could be influenced by the type of material of the footwear.
We consider the small sample size as the main limitation of this study compared to similar studies(20). This could be one of the reasons why a decrease in plantar pressures was obtained in the control group. As mentioned above, increasing the sample size could homogenize the groups and obtain better results. Other limitations found was the fact that feet were counted instead of people. In case that a participant has not respected the researchers’ instructions to perform the exercises, the impact will have been in 2 cases (2 feet) instead of one. It would be interesting to include only one foot per person in future studies.
In conclusion, in this study it was observed that the subjects who performed an exercise program with elastic bands to strengthen the PL muscle after four weeks of training presented an increase in plantarflexion of the first ray (from 3.81 to 4 .50 mm; p = 0.016); an increase in the pressure of the first metatarsal head during the stance phaseof gait (from 7.64 to 11.55 N/cm2) and its maximum pressure in dynamics (from 22.07 to 31.32 N /cm2); an increase in the percentage of the time interval in which this maximum pressure occurs during the stance phase (from 77.96 to 79.76); and a decrease in the percentage of loading time during the stance phase (from 79.24 to 76.30 %).
Ethics declaration
This research complies with current regulations on bioethics and respects the principles of the Declaration of Helsinki (World Medical Assembly), the Council of Europe Convention on Human Rights, and the UNESCO Declaration on Human Rights. and was approved bythe Clinical Research Ethics Committee of the University of Seville (ID: 0498-N23). All participants gave signed consent before being included in the study. Authorization was also obtained from the Podiatry Clinical Area of the University of Seville. This clinical trial has a registration number in ClinicalTrials.gov (NCT05647616).
Conflict of interest
The authors declare no conflicts of interest regarding this paper.
Funding
None.
Authors contribution
Conception and design: PTV, MJMM.
Data collection: PTV.
Results analysis: PTV.
Creation and redation of initical draft: PTV, MJMM.
Final Review: PTV, MJMM.
References
- Munuera PV. El primer radio. Biomecánica y Ortopodología. 2.ª ed. Santander: Exa Editores SL; 2012.
- Wong DW chi, Zhang M, Yu J, Leung AKL. Biomechanics of first ray hypermobility: an investigation on joint force during walking using finite element analysis. Med Eng Phys. 2014;36(11):1388-93. DOI: 10.1016/j.medengphy.2014.03.004.
- Glasoe W, Yack HJ, Saltzman CL. Anatomy and biomechanics of the first ray. Phys Ther. 1999;79(9):854-9. DOI: 10.1093/ptj/79.9.854.
- Root M, Orien W, Weed J. Normal and abnormal function of the foot, vol 2. Los Angeles: Clinical Biomechanics Corp; 1977.
- Rueda M. Introducción a la biomecánica del pie (VI). Apunts Med Esport. 2005; 146:37-41. DOI: 10.1016/S1886-6581(05)76097-7.
- Rico R. Biomecánica del Primer Radio. Deformidad en flexión plantar. Caso clínico. Rev Int Cienc Podol. 2008;3(1):53-66.
- Bierman RA, Christensen JC, Johnson CH. Biomechanics of the first ray. Part III. Consequences of lapidus arthrodesis on peroneus longus function: A three-dimensional kinematic analysis in a cadaver model. J Foot Ankle Surg. 2001;40(3):125-31. DOI: 10.1016/S1067-2516(01)80077-6.
- Johnson CH, Christensen JC. Biomechanics of the first ray Part I. The effects of peroneus longus function: A three-dimensional kinematic study on a cadaver model. J Foot Ankle Surg. 1999;38(5):313-21. DOI: 10.1016/S1067-2516(99)80002-7.
- Roca-Dols A, Losa-Iglesias ME, Sánchez-Gómez R, López-López D, Becerro-de-Bengoa-Vallejo R, Calvo-Lobo C. Electromyography comparison of the effects of various footwear in the activity patterns of the peroneus longus and brevis muscles. J Mech Behav Biomed Mater. 2018;82:126-32. DOI: 10.1016/j.jmbbm.2018.03.003.
- Dullaert K, Hagen J, Klos K, Gueorguiev B, Lenz M, Richards RG, et al. The influence of the Peroneus Longus muscle on the foot under axial loading: A CT evaluated dynamic cadaveric model study. Clin Biomech. 2016;34:7-11. DOI: 10.1016/j.clinbiomech.2016.03.001.
- Choi Y, Lee J. Effect of peroneus longus muscle release on abductor hallucis muscle activity and medial longitudinal arch before toe-tap exercise in participants with flexible pes planus. Healthcare. 2021;10(44):1-9. DOI: 10.3390/healthcare10010044.
- Duchenne G. Physiologie des Mouvements. Philadelphia: Lippincott Williams and Wilkins; 1867.
- 1Sánchez Gómez R, De Benito González S, Gómez Martín B, Álvarez-Calderón Iglesias O, Rico Teixeira R. Maniobra de fiabilidad para el Músculo Peroneo Lateral Largo: Hipermobilidad del Primer Radio. Rev Int Cienc Podol. 2009;3(1):35-44.
- Cornwall MW, Fishco WD, McPoil TG, Lane CR, O’Donnell D, Hunt L. Reliability and validity of clinically assessing first-ray mobility of the foot. J Am Podiatr Med Assoc. 2004;94(5):470-6. DOI: 10.7547/0940470.
- Wang H, Yu H, Kim YH, Kan W. Comparison of the effect of resistance and balance training on isokinetic eversion strength, dynamic balance, hop test, and ankle score in ankle sprain. Life. 2021;11(4)1-13. DOI: 10.3390/life11040307.
- Song SH, Park JH, Song GD, Lee SG, Jo YH, Jin MK, et al. Usability of the Thera-Band® to improve foot drop in stroke survivors. NeuroRehabilitation. 2018;42(4):505-10. DOI: 10.3233/NRE-172338.
- Spencer Cain M, Ban RJ, Chen YP, Geil MD, Goerger BM, Linens SW. Four-week ankle-rehabilitation programs in adolescent athletes with chronic ankle instability. J Athl Train. 2020;55(8):801-10. DOI: 10.4085/1062-6050-41-19.
- Kaminski TW, Buckley BD, Powers ME, Hubbard TJ. Effect of strength and proprioception training on eversion to inversion strength ratios in subjects with unilateral functional ankle instability. Br J Sports Med. 2003;37(5):410-5. DOI: 10.1136/bjsm.37.5.410.
- Begg C, Cho M, Eastwood S, Horton R, Olkin I. Improving the quality of reporting of randomized controlled trials. The CONSORT statement. JAMA. 1996;276(8):637-9. DOI: 10.1001/jama.1996.03540080059030.
- Munuera-Martínez PV, Távara-Vidalón P, Monge-Vera MA, Sáez-Díaz A, Lafuente-Sotillos G. The validity and reliability of a new simple instrument for the measurement of first ray mobility. Sensors. 2020;20(8):1-16. DOI: 10.3390/s20082207.
- Távara-Vidalón P, Lafuente-Sotillos G, Munuera-Martínez PV. Movimiento del primer dedo en sujetos con hallux limitus vs. sujetos con pies normales. Rev Esp Podol. 2021;32(2):116-
- DOI: 10.20986/revesppod.2021.1621/2021.
- Távara-Vidalón P, Lafuente-Sotillos G, Manfredi-Márquez MJ, Munuera-Martínez PV. Movilidad normal del primer radio en los planos sagital y frontal. Rev Esp Podol. 2021;32(1):27-35. DOI: 10.20986/revesppod.2021.1600/2021.
- Redmond AC, Crosbie J, Ouvrier RA. Development and validation of a novel rating system for scoring standing foot posture: The Foot Posture Index. Clin Biomech. 2006;21(1):89-98. DOI: 10.1016/j.clinbiomech.2005.08.002.
- Martínez-Nova A, Sánchez-Rodríguez R, Cuevas-García JC, Sánchez-Barrado E. Estudio baropodométrico de los valores de presión plantar en pies no patológicos. Rehabilitación. 2007;41(4):155-60. DOI: 10.1016/S0048-7120(07)75509-3.
- Martínez-Nova A, Cuevas-García JC, Sánchez-Rodríguez R, Pascual-Huerta J, Sánchez-Barrado E. Estudio del patrón de presiones plantares en pies con hallux valgus mediante un sistema de plantillas instrumentadas. Rev Esp Cir Ortop Traumatol. 2008;52(2):94-8. DOI: 10.1016/S1888-4415(08)74801-X.
- Cain MS, Ban RJ, Chen YP, Geil MD, Goerger BM, Linens SW. Four-week ankle-rehabilitation programs in adolescent athletes with chronic ankle instability. J Athl Train. 2020;55(8):801-10. DOI: 10.4085/1062-6050-41-19.
- Cohen J. Statistical Power Analysis for the Behavioral Sciences. 2.nd ed. Abingdon, Inglaterra: Routledge; 1988. p. 567.
- Tavara-Vidalón P, Monge-Vera M, Lafuente-Sotillos G, Domínguez-Maldonado G, Munuera-Martínez P. Static range of motion of the first metatarsal in the sagittal and frontal planes. J Clin Med. 2018;7(11):456. DOI: 10.3390/jcm7110456.
- Landis J, Koch G. The measurement of observer agreement for categorical data. Biometrics. 1977;33(1):159-74. DOI: 10.2307/2529310.
- Murley GS, Menz HB, Landorf KB. Foot posture influences the electromyographic activity of selected lower limb muscles during gait. J Foot Ankle Res. 2009;2(1):35. DOI: 10.1186/1757-1146-2-35.
- Thordarson D, Schmotzer H, Chon J, Peters J. Dynamic support of the human longitudinal arch. A biomechanical evaluation. Clin Orthop Relat Res. 1995;316:165-72. DOI: 10.1097/00003086-199507000-00022.
- McLoda TA, Hansen AJ. Effect of a task failure exercise on the peroneus longus and brevis during perturbed gait. Electromyogr Clin Neurophysiol. 2005;45:53-8.
- Bavdek R, Zdolšek A, Strojnik V, Dolenec A. Peroneal muscle activity during different types of walking. J Foot Ankle Res. 2018;11(1):50. DOI: 10.1186/s13047-018-0291-0.
- Ha S, Fong D, Chan K. Review of ankle inversion sprain simulators in the biomechanics laboratory. Asia Pac J Sports Med Arthrosc Rehabil Technol. 2015;2(4):114-21. DOI: 10.1016/j.asmart.2015.08.002.
- Peng HT, Song CY, Chen ZR, Lai CT, Gu CY, Wang LI. Effects of attaching elastic bands to the waist and heels on drop jumps. Eur J Sport Sci. 2022;22(6):808-16. DOI: 10.1080/17461391.2021.1915390.
- Veneri D. Combining the treatment modalities of body weight support treadmill training and thera-band: A case study of an individual with hemiparetic gait. Top Stroke Rehabil. 2011;18(4):402-16. DOI: 10.1310/tsr1804-402.
- Yu W, An C, Kang H. Effects of resistance exercise using thera-band on balance of elderly adults: a randomized controlled trial. J. Phys Ther Scl. 2013;25:1471-3. DOI: 10.1589/jpts.25.1471.
- Patil P, Rao SA. Effects of Thera band elastic resistance-assisted gait training in stroke patients. Eur J Phys Rehabil Med. 2011;47(3):427-33.
- Choi SA, Cynn HS, Yi CH, Kwon OY, Yoon TL, Choi WJ, et al. Isometric hip abduction using a Thera-Band alters gluteus maximus muscle activity and the anterior pelvic tilt angle during bridging exercise. J Od Electromyogr Kinesiol. 2015;25:310-5. DOI: 10.1016/j.jelekin.2014.09.005.
- Ludwig O, Kelm J, Fröhlich M. The influence of insoles with a peroneal pressure point on the electromyographic activity of tibialis anterior and peroneus longus during gait. J Foot Ankle Res. 2016;9(1):33. DOI: 10.1186/s13047-016-0162-5heels on drop jumps. Eur J Sport Sci. 2022;22(6):808-16.