DOI: 10.20986/revesppod.2022.1627/2021
ORIGINAL
Baropodometric variation with weight loss: an experimental study
Variación baropodométrica con la pérdida de peso: un estudio experimental
Carla Lanuza-Cerzócimo1,2
Javier Alfaro-Santafé1,2
Alejandro Jesús Almenar-Arasanz2
José V. Alfaro-Santafé1,2
Aitor Pérez-Morcillo2
Antonio Gómez-Bernal1,2
1Central University of Catalonia. Manresa, Barcelona, Spain. 2Research Department of Podoactiva. Huesca, Spain
Abstract
Objective: One of the major public health problems of the 21st century is obesity. Baropodometry is commonly used to determine specific loads on the plantar surface of the foot and the behaviour of the body center of pressure (CoP). The aim of the present investigation was to evaluate the redistribution of the baropodometric parameters: static and dynamic plantar pressures and anteroposterior CoP, as body weight decreased.
Patients and methods: A sample of 43 subjects (24male, 19 female) participated in the study. A hypocaloric diet was designed with the aim to reduce their body weight. The baropodometric exam was performed in two occasions: weight 1 – Session 1 and weight 2 – Session 2, when they had lost between 12 and 18 kg. The foot was divided in 9 areas: heel, midfoot, 5 metatarsal heads (MTHs), Hallux, 2-5 toes. The Footwork® pressure platform was used to carry out the evaluation.
Results: Subjects reduce an 11.59 % their mean weight. Foot pressure decrease was statistically significant between the first and second measurements (p < 0.05). For the static on the Hallux, 2nd MTH, 3rd MTH, 5th MTH and heel, while for the dynamic the pressure decreases on the whole study areas except on the 2nd and 5th toes. For the CoP, a notable posterior displacement was observed. There were no gender differences.
Conclusions: We can conclude that weight loss affected positively to both plantar pressures and CoP, since statistically significant changes were observed in the baropodometric parameters between the two times studied.
Keywords: Static, dynamic, postural imbalance, pressure, obesity, plantar pressures, baropodometry
Resumen
Objetivos: Uno de los principales problemas de salud pública del siglo xxi es la obesidad. La baropodometría se utiliza habitualmente para determinar las cargas específicas sobre la superficie plantar del pie y el comportamiento del centro de presión corporal (CoP). El objetivo de la presente investigación fue evaluar la redistribución de los parámetros baropodométricos: presiones plantares estáticas y dinámicas y CoP anteroposterior, al disminuir el peso corporal.
Pacientes y métodos: Una muestra de 43 sujetos (24 hombres y 19 mujeres) participaron en el estudio. Se diseñó una dieta hipocalórica con el objetivo de reducir su peso corporal. El examen baropodométrico se realizó en dos ocasiones: peso 1 - Sesión 1 y peso 2 - Sesión 2, cuando habían perdido entre 12 y 18 kg. El pie se dividió en 9 zonas: talón, mediopié, 5 cabezas metatarsales (MTH), hallux, 2-5 dedos. Se utilizó la plataforma de presión Footwork® para realizar la evaluación.
Resultados: Los sujetos reducen un 11.59 % su peso medio. La disminución de la presión del pie fue estadísticamente significativa entre la primera y la segunda medición (p < 0.05). Para la estática en el Hallux, 2.º MTH, 3.º MTH, 5.º MTH y talón, mientras que para la dinámica la presión disminuye en todas las zonas de estudio excepto en el 2.º y 5.º dedo. Para el CoP se observó un notable desplazamiento posterior. No hubo diferencias de género.
Conclusiones: Podemos concluir que la pérdida de peso afectó positivamente tanto a las presiones plantares como a la CoP, ya que se observaron cambios estadísticamente significativos en los parámetros baropodométricos entre los dos momentos estudiados.
Palabras clave: Estática, dinámica, desequilibrio postural, presión, obesidad, presiones plantares, podobarometría
Received: 22-12-2021
Accepted: 08-02-2022
Correspondence: Antonio Gómez-Bernal
antoniogomez@podoactiva.com
INTRODUCTION
Obesity is in one of the major public health problems of the 21st century and its prevalence has tripled in many European countries in the last decades1. It is a strong problem associated with a lower quality of life, as well as with the development of serious chronic metabolic, cardiac and circulatory problems and musculoskeletal disorders2,3. Quantitative data showed that excessive body weight negatively effects on standing and walking4,5. Plantar pressure measurement is commonly used to determine specific loads on the plantar surface of the foot. There are many case studies that assess pressures of the normal foot and try to establish patterns of pathological pressures6. The center of pressure (CoP) represents the average of all the weight that is in contact with the surface of the floor and is expressed as the point where the vector of the vertical reaction forces of the soil is located6,7.
In the literature it can be found how body weight influences on plantar pressure data and on the position of the CoP8-10. Excesses of body weight has shown to have negative structural consequences in the feet and lower limbs, it increases the possibilities of suffereing of plantar fasciitis or knee arthrosis among others11-14. Obesity is also related with an anterior displacement of the CoP15, since the instability in obese people, associated to weight increasing, seems to be determinant with CoP in an anterior position16.
Computerized baropodometry (plantar pressure measurement) is helpful for foot diseases diagnosis, foot function evaluation and to follow-up the treatment. It has been practiced to determine specific weight parameters in obese adults, among others10,14. Nonetheless, there are not in the literature specific studies that have analyzed by computerized baropodometry how plantar pressures and CoP improve by decreasing body weight in obese adults.
Therefore, with this study we aim to evaluate plantar pressures and antero – posterior CoP improvement by decreasing body weight in static and dynamic baropodometry data collection in obese adults.
PATIENTES AND METHODS
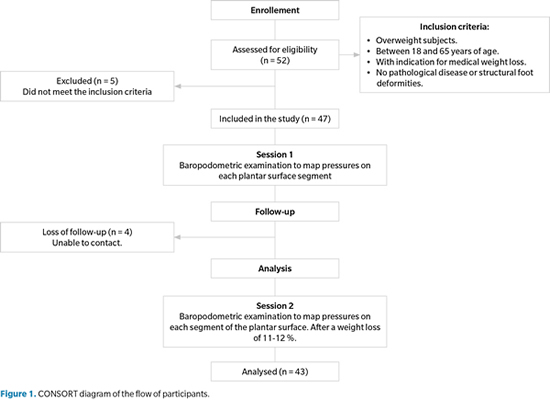
Between June 2009 and December 2009, we conducted a controlled experimental study. This was designed to investigate whether a decrease in body weight in obese individuals has a variation in plantar and antero-posterior CoP pressures, through a controlled intervention over a specific period of time aimed at achieving this decrease in total body weight for each individual. The participants chosen for the protocol, specifically, 43 adults with diagnosed obesity, had to present themselves at the clinic on two occasions. On the first occasion (Session 1) participants were assessed by the podiatric phycisian and the endocrinoslogist prior to the intervention, and on the second occasion (Session 2) participants were again assessed after the weight loss intervention by the same doctors. The design of the present research was based on and executed according to the CONSORT reporting guideline.
Participants
Participants were recruited at one Endocrinology and Nutrition private clinic in Huesca, Spain. Fifhty-two subjects were recruited, of whom five were excluded because they did not meet the inclusion criteria. At the start of the study, 47 participants were recruited, of which 4 could not be contacted again. Finally, the study was conducted on a sample of 43 patients (Figure 1), 24 were men and 19 women, mean age 48 ± 12.6 years (range, 19-64 years), apparently without pathological gait disease or severe structural or functional deformities in the feet. Inclusion criteria included overweight subjects between 18 and 65 years old, medical weight loss indicated, no lower limb or spine pathology that might affect normal gait, nor structural or functional deformities in the feet. Candidates who did not comply inclusion criteria or reported pain in their feet within the previous 6 months or had any previous foot surgery were excluded.
Experimental protocol and evaluation plan
Participants were rigorously evaluated by the same endocrine doctor and podiatrist at baseline (Session 1) and at the end of the study after weight loss intervention (Session 2), when each participant had lost between 11-12 % of its corporal weight. Therefore, we obtained 2 weight related with the two sessions: Session 1 – Weight 1; Session 2 – Weight 2.
In order to achieve the proposed weight loss, lifestyle modification was applied17: A specific very low-calorie diet (< 800 kcal/day), and 2 daily sessions of 15 minutes of anaerobic physical exercise depending on the capacity of the participants, were designed by an experienced endocrinology18,19.
At Session 1 and Session 2, before and after weight loss intervention, participants were subjected to a baropodometric examination (static and dynamic). It allowed to quantitatively mapping pressures in each segment of the plantar surface20,21. For the static, participants were asked to stand in the center of the platform for 5 seconds, with their arms on either side of the body in a natural position looking straight ahead22. To minimize individual´s corporal fluctuations in static (as body weight oscillation and imbalance) we applied this procedure 3 times per session22. For the dynamic, participants were asked to walk barefoot on the platform at their normal pace following the 3-step protocol, which requires landing on the platform on the third step of gait23. To minimize individual’s corporal fluctuations in dynamic (as body weight oscillation, imbalance and changes in gait speed) we applied this procedure 3 times per session22. Both feet were subdivided into 9 areas: heel, midfoot, 5 MTHs, the Hallux, 2-5 toes (Figure 2). Selection of the areas of the present study is justified because it is based on the daily clinic, where the consultations of overweight patients are usually due to discomfort or pain in metatarsal heads (MTH), reason why these are studied separately and is supported by authors like Hills et al.11, who performed a complete study of the differences of pressures between obese and non-obese subjects.
Peak pressures of these areas in kg/cm2 and the position of the CoP, were obtained using the Footwork® software20. Peak pressure data were graphically exposed and related with the two weights for each patient.

Equipment
Footwork® platform (AM3-IST®, France), was used for the baropodometric analysis22,24 (Figure 3). Participant´s weight and height were measured during each session with an Año-Sayol scale and stadiometer, respectively (Año-Sayol SL, Barcelona, Spain).
Statistical analysis and study variables
An initial exploratory analysis of all clinical variables was carried out. Continuous variables were expressed as mean ± standard deviation (SD), whereas qualitative variables were expressed as frequencies and percentages. Continuous data were checked for normality by Kolmogorov-Smirnov Test. Chi-Square Test was applied to show the relationship between qualitative variables. To compare mean weights between two independent groups according to normality, we used Student’s t test. Differences between Session 1 and Session 2, were performed using mean comparison methods, Wilcoxon when the variable did not follow normal distribution, and t-Student for related samples when there was normality. To quantify the difference between weight and plantar pressures and the CoP at Session 1 and Session 2 the “change percentage” was calculated, which was defined as the relative variation in percentage points between both sessions: Weight-Change % (WC %) = [(Weight at Session 2 – Weight at Session 1) / Weight Session 1] x 100; Plantar-Pressure-Change % (PPC %) = [(Pressure at Session 2 – Pressure at Session 1) / Pressure at Session 1] x 100; CoP-Change % = [(time CoP X+1 – time CoP X) / time CoP X] x 100. The “change percentage” was analyzed through Spearman correlation coefficient, according to normality.
The “improve” variable was established in order to analyze the possible relationship between weight loss and the 9 pressure foot areas considered at Session 1 and Session 2 for both: static and dynamic baropodometry. Statistical significance level was set at p < 0.05 and confidence level at 95 % was also calculated. The statistical analyses were performed using the SPSS software 22.0 for Windows (IBM Corp. Version 22.0. Armonk, NY, USA).

RESULTADOS
All participants came from Endocrinology and Nutrition consultation and were overweight: mean weight for men 87 (range, 72-104) kg and 68 (range, 62-75) kg for women, with a Body Mass Index (BMI) higher than 25. The mean comparison of the two weights studied is shown in Table I. The loss of weights between both times was statistically significant (p < 0.05). As well there can be observed the weight differences between genders which had no statistical significance.
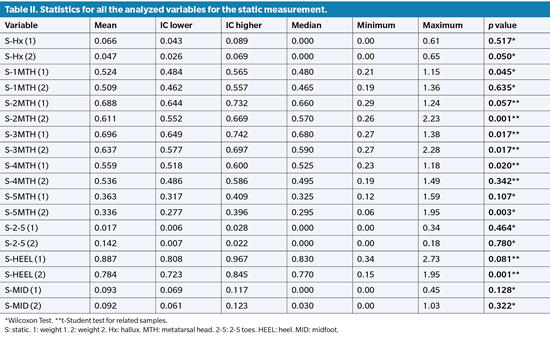
For the plantar pressures, in static (Table II) a statistically significant mean pressure decrease between the first and the second measurement on the Hallux, 2nd MTH, 3rd MTH, 5th MTH and heel was observed.
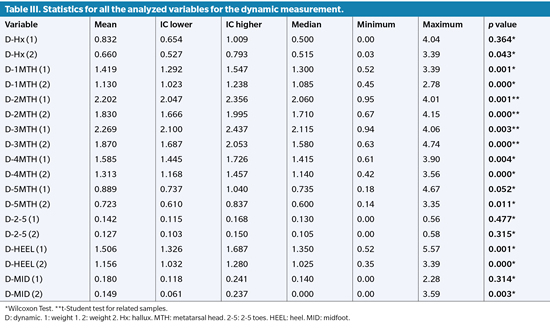
In dynamic (Table III) a statistically significant pressure decrease between the first and second measurements on the Hallux, 1st MTH, 2nd MTH, 3rd MTH, 4th MTH, 5th MTH, heel and midfoot was observed. In summary all study areas except in the 2nd to 5th toes.
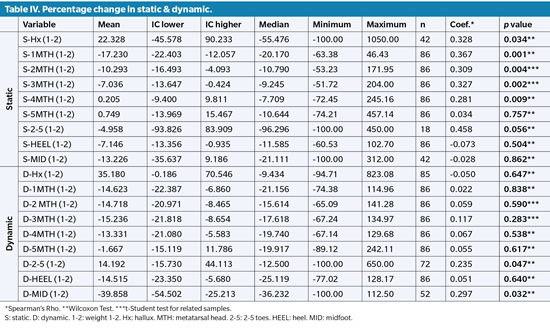
Table IV shows the descriptive analysis, as well as the number of patients (n) considered in each case. The relationship between weight change and pressure change was studied using the Spearman correlation coefficient. In static, it is observed that the weight variation is statistically significant in the pressures of the Hallux, 1st MTH, 2nd MTH, 3rd MTH and 4th MTH. In dynamics between Session 1 and Session 2we found only a significant association between pressure changes and weight variation in the 2nd to 5th toes and midfoot.

DISCUSSION
Changes in long - term posture, such as those produced by weight gain, may induce permanent degenerative changes in the musculoskeletal system25. Therefore, weight loss, will influence positively body posture, which can be observed by studying plantar pressure and the movement of the CoP26.
In the present research there have been no significant changes between the variation of the CoP and the gender, as evidenced by Rogind et al.27 and Nordahl et al.28. But we have observed that the CoP moves backwards when losing weight. These results match with those obtained by DeVita et al.29, who demonstrated that the CoP displaces forwards when weight increases. Gilleard and Smith in 200716, emphasized this and added the hypothesis of the lack of stability in obese as a determinant of anterior displacement.
Obesity has been associated with greater forward movement of the center of pressures15. Body mass gain in obese people generates an instability increasing which leads to a major muscular response to maintain the CoP in the center of the support polygon. The location of the fat mass in the body (thorax-abdominal in men; hips in women) contributes to the antero-posterior instability30.
In the literature we find opposite opinions about the influence of the weight in plantar pressure values. Several studies agreed that there is a direct correlation between both factors11-13, i.e. weight influences plantar pressures, which has structural consequences in the feet and lower limbs11.
Our findings showed that when weight decreased statistically significant differences were found on the MTHs in static and on the midfoot in dynamics31. These findings are supported by Birtane et al.32, who demonstrated that weight gain does not increase peak pressures of the forefoot walking, although it was found that the most sensitive anatomical area was 1st MTH where it was observed that weight gain increases peak pressures13.
In the study of Arnold et al.33, they observed the correlation between higher plantar pressures when weight increases. There were studied three times: when subjects increase 5, 10 and 15 kg, being found the relation for the two latest weights on the Hallux, every MTHs and heel.
Riddiford-Harland et al.34, justifies the fact that the middle zone is the most sensitive to pressure change due to the increase in the impact forces that limit the capacity of the medial longitudinal arch to attenuate this change and therefore the adaptation occurs by increase the support of the middle part of the foot34. Arnold et al.33 manifests that in his study this area does not appear as statistically significant because weight gains only reached up to 15 kg, our study does not support this hypothesis since the weight loss oscillated between 5.5 and 13.2 kg and this was the only statistically significant area along with the toes.
In the case of Hills et al. it was noted that the most notable increase in peak pressure among non-obese and obese occurred on the middle region of the foot. Their study coincides with our data but with large differences in the mean of body mass between obese and non-obese subjects, 36.0 kg for women and 43.6 kg for men11. Arnold bases his foundation on this study, that a greater variance in weight between both groups (obesity and non-obesity) more significant the difference on the middle zone33.
The results of the present study can be related with those of Song et al.35 and Mueller et al.13, who defend that when the weight increases the plantar arch descends (more in pronated foot) increasing the load on the medial surface of the foot´s sole, coinciding with our study.
One limitation of the present research should be highlighted, the lateral movement of the CoP was no considered. Anyway, the findings of this work reveal the important relationship between weight and musculoskeletal system.
We can conclude that weight loss positively affects the static CoP and plantar pressures, both static and dynamic, since there is observed statistically significant changes on antero – posterior CoP and plantar pressures between the two times studied. CoP moves backwards which means balance and healthy postural gain, it should be noted that weight reduction affects differently static and dynamic plantar pressures. We can observe that there is no anatomical area of the 9 studied which coincides between static and dynamic studies as statistically significant.
ETHICS DECLARATION
Ethics approval and consent to participate: the study was approved by the Ethics Committee of Clinical Research of Aragón (C.P.-C.I.PI17/0203)
AVAILABILITY OF DATA AND MATERIALS
The datasets used and/or analysed during the current study are available from the corresponding author on reasonable request.
COMPETING INTEREST
The authors declare that they have no competing interests.
FUNDING
Not applicable.
AUTHOR'S CONTRIBUTION
CL-C had the original idea for this research, designed the protocol, evaluated the patients and designed the treatment. AG-B evaluated patients at baseline and after follow-up. JA-S performed the statistical analysis of the data. JVA-S performed the statistics. AP-M reviewed and drafted the manuscript, AJA-A reviewed and drafted the manuscript.
REFERENCES
- Monastir L, Batty GD, Cattaneo A, Lutje V, Ronfani L, Van Lenthe FJ, et al. Early-life determinants of overweight and obesity: a review of systematic reviews. Obes Rev. 2010;11(10):695-708. DOI: 10.1111/j.1467-789X.2010.00735.x.
- Buckley J. Exercise self-efficacy intervention in overweight and obese women. J Health Psychol. 2016;21(6):1074-84. DOI: 10.1177/1359105314545096.
- Benítez-Andrades JA, Arias N, García-Ordás MT, Martínez-Martínez M, García-Rodríguez I. Feasibility of Social-Network-Based eHealth Intervention onthe Improvement of Healthy Habits among Children. Sensors (Basel). 2020;20(5). pii: E1404. DOI: 10.3390/s20051404.
- de Souza SA, Faintuch J, Valezi AC, Sant’ Anna AF, Gama-Rodrigues JJ, de Batista Fonseca IC, et al. Gait cinematic analysis in morbidly obese patients. Obes Surg. 2005;15(9):1238-42. DOI: 10.1381/096089205774512627.
- Vismara L, Romei M, Galli M, Montesano A, Baccalaro G, Crivellini M, et al. Clinical implications of gait analysis in the rehabilitation of adult patients with “Prader-Willi” Syndrome: a cross-sectional comparative study (“Prader-Willi”Syndrome vs matched obese patients and healthy subjects). J Neuroeng Rehabil. 2007;4:14. DOI: 10.1186/1743-0003-4-14.
- Lee W, Hong SH, Oh HW. Characterization of Elastic Polymer-Based Smart Insoleand a Simple Foot Plantar Pressure Visualization Method Using 16 Electrodes. Sensors (Basel). 2018;19(1). pii: E44. DOI: 10.3390/s19010044.
- Gomez Bernal A, Becerro-de-Bengoa-Vallejo R, Losa-Iglesias ME. Reliability of the OptoGait portable photoelectric cell system for the quantification of spatial-temporal parameters of gait in young adults. Gait Posture. 2016;50:196-200. DOI: 10.1016/j.gaitpost.2016.08.035.
- Ferrin B, Diego C, Magdalena X, Correa HL. Determinación semiautomática de parámetros morfológicos de la huella plantar mediante el procesamiento digital de imágenes. Sistemas & Telemática. 2013;11(27):9-26.
- Puig-Diví A, Prats-Puig A. Postural and dynamic analysis of the human body: The relevance of the functional modulator factors in the methodological design. Mult J Educ Soc & Tec Sci. 2015;2(2):95-120. DOI: 10.4995/muse.2015.3754.
- Wafai L, Zayegh A, Woulfe J, Aziz SM, Begg R. Identification of Foot Pathologies Based on Plantar Pressure Asymmetry. Sensors (Basel). 2015;15(8):20392-408. DOI: 10.3390/s150820392.
- Hills AP, Hennig EM, McDonald M, Bar-Or O. Plantar pressure differences between obese and non-obese adults: a biomechanical analysis. Int J Obes Relat Metab Disord. 2001;25(11):1674-9. DOI: 10.1038/sj.ijo.0801785.
- Menz HB, Morris ME. Clinical determinants of plantar forces and pressures during walking in older people. Gait Posture. 2006;24(2):229-36. DOI: 10.1016/j.gaitpost.2005.09.002.
- Mueller MJ, Hastings M, Commean PK, Smith KE, Pilgram TK, Robertson D, Johnson J. Forefoot structural predictors of plantar pressures during walking in people with diabetes and peripheral neuropathy. J Biomech. 2003;36(7):1009-17. DOI: 10.1016/S0021-9290(03)00078-2.
- Taborri J, Palermo E, Rossi S, Cappa P. Gait Partitioning Methods: A Systematic Review. Sensors (Basel). 2016;16(1). pii: E66. DOI: 10.3390/s16010066.
- Berrigan F, Simoneau M, Tremblay A, Hue O, Teasdale N. Influence of obesity on accurate and rapid arm movement performed from a standing posture. Int J Obes (Lond). 2006;30(12):1750-7. DOI: 10.1038/sj.ijo.0803342.
- Gilleard W, Smith T. Effect of obesity on posture and hip joint moments during a standing task, and trunk forward flexion motion. Int J Obes (Lond). 2007;31(2):267-71. DOI: 10.1038/sj.ijo.0803430.
- Fujioka K. Benefits of moderate weight loss in patients with type 2 diabetes. Diabetes Obes Metab. 2010;12(3):186-94. DOI: 10.1111/j.1463-1326.2009.01155.x.
- Siram AT, Yanagisawa R, Skamagas M. Weight management in type 2 diabetes mellitus. Mt Sinai J Med. 2010;77(5):533-48. DOI: 10.1002/msj.20208.
- Anderson JW, Kendall CW, Jenkins DJ. Importance of weight management in type 2 diabetes: review with meta-analysis of clinical studies. J Am Coll Nutr. 2003;22:331-9. DOI: 10.1080/07315724.2003.10719316.
- Fabris SM, Valezi AC, de Souza SA, Faintuch J, Cecconello I, Junior MP. Computerized baropodometry in obese patients. Obes Surg. 2006;16(12):1574-8. DOI: 10.1381/096089206779319293.
- Gravante G, Russo G, Pomara F, Ridola C. Comparison of ground reaction forces between obese and control young adults during quiet standing on a baropodometric platform. Clin Biomech (Bristol, Avon). 2003;18(8):780-2. DOI: 10.1016/S0268-0033(03)00123-2.
- Becerro de Bengoa Vallejo R, Losa Iglesias ME, Zeni J, Thomas S. Reliability and repeatability of the portable EPS-platform digital pressure-plate system. J Am Podiatr Med Assoc. 2013;103(3):197-203. DOI: 10.7547/1030197.
- Peter EJG, Urukalo A, Fleischli JG, Lavery LA. Reproducibility of Gait Analysis Variables: One-Step versus Three-Step Method of Data Acquisition. J Foot Ankle Surg. 2002;41(4):206-12. DOI: 10.1016/S1067-2516(02)80016-3.
- Giacomozzi C. Appropriateness of plantar pressure measurement devices: a comparative technical assessment. Gait Posture. 2010;32(1):141-4. DOI: 10.1016/j.gaitpost.2010.03.014.
- Hue O, Simoneau M, Marcotte J, Berrigan F, Doré J, Marceau P, Marceau S,Tremblay A, Teasdale N. Body weight is a strong predictor of postural stability. Gait Posture. 2007;26(1):32-8. DOI: 10.1016/j.gaitpost.
2006.07.005.
- Ruhe A, Fejer R, Walker B. The test-retest reliability of centre of pressure measures in bipedal static task conditions-a systematic review of the literature. Gait Posture. 2010;32(4):436-45. DOI: 10.1016/j.gaitpost.
2010.09.012.
- Røgind H, Lykkegaard JJ, Bliddal H, Danneskiold-Samsøe B. Postural sway in normal subjects aged 20-70 years. Clin Physiol Funct Imaging. 2003;23(3):171-6. DOI: 10.1046/j.1475-097X.2003.00492.x.
- Nordahl SH, Aasen T, Dyrkorn BM, Eidsvik S, Molvaer OI. Static stabilometry and repeated testing in a normal population. Aviat Space Environ Med. 2000;71(9):889-93.
- DeVita P, Hortobágyi T. Obesity is not associated with increased knee joint torque and power during level walking. J Biomech. 2003;36(9):1355-62. DOI: 10.1016/S0021-9290(03)00119-2.
- Clark KN. Balance and strength training for obese individuals. ACSM’s Health & Fitness J. 2004;8(1):14-20. DOI: 10.1097/00135124-200401000-00008.
- Bolte K, Hennig E, Hills A, McDonald M. Pressure changes under the feet of obese adults after a weight reduction program. Arch Physiol Biochem. 2000;108(1-2):70.
- Birtane M, Tuna H. The evaluation of plantar pressure distribution in obese and non-obese adults. Clin Biomech. 2004;19(10):1055-9. DOI: 10.1016/j.clinbiomech.2004.07.008.
- Arnold JB, Causby R, Dip Pod G, Jones S. The impact of increasing body mass on peak and mean plantar pressure in asymptomatic adult subjects during walking. Diabetic foot & ankle. 2010;1(1):5518. DOI: 10.3402/dfa.v1i0.5518.
- Riddiford-Harland DL, Steele JR, Storlien LH. Does obesity influence foot structure in prepubescent children? Int J Obes Relat Metab Disord. 2000;24(5):541-4. DOI: 10.1038/sj.ijo.0801192.
- Song J, Kane R, Tango DN, Vander Veur SS, Furmato J, Komaroff E, et al. Effects of weight loss on foot structure and function in obese adults: a pilot randomized controlled trial. Gait Posture. 2015;41(1):86-92. DOI: 10.1016/j.gaitpost.2014.08.013.